
Get the free Patient Request Form - vfce arizona
Show details
This document is intended for patients to request referrals related to Valley Fever, capturing essential personal information, medical history, and contact details.
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign patient request form
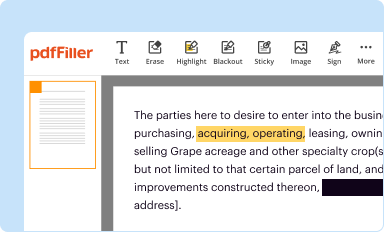
Edit your patient request form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
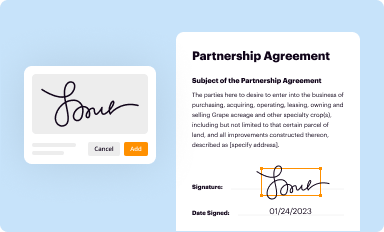
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
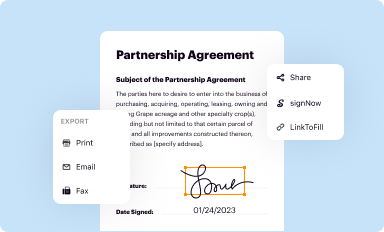
Share your form instantly
Email, fax, or share your patient request form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing patient request form online



Follow the guidelines below to benefit from the PDF editor's expertise:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit patient request form. Add and replace text, insert new objects, rearrange pages, add watermarks and page numbers, and more. Click Done when you are finished editing and go to the Documents tab to merge, split, lock or unlock the file.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
The use of pdfFiller makes dealing with documents straightforward.
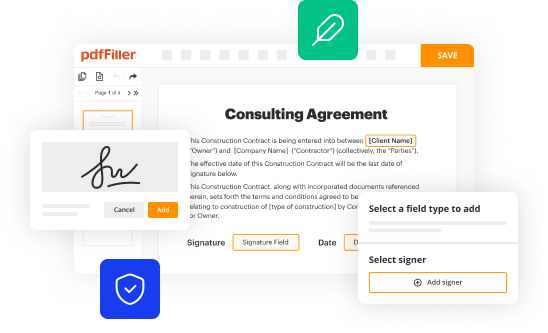
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out patient request form
How to fill out Patient Request Form
01
Obtain the Patient Request Form from your healthcare provider's office or website.
02
Fill in your personal information, including your full name, date of birth, and contact details.
03
Provide the details of the medical records or information you are requesting.
04
Include the reason for your request if required by the form.
05
Sign and date the form to certify that the information is accurate.
06
Submit the completed form to the designated office, either in person or through email/fax as instructed.
Who needs Patient Request Form?
01
Patients who wish to access their medical records.
02
Individuals seeking information on diagnoses, treatments, or test results.
03
Parents or guardians requesting records on behalf of their minor children.
04
Patients transferring their records to new healthcare providers.
Fill
form
: Try Risk Free
People Also Ask about
What is a clinical request?
Clinical Requests - The researcher wants to request access to data from only the hospital he/she is affiliated with, for the research purpose for which the study was originally designed.
What is a patient triage request?
Triage, where patient requests are screened by the practice and signposted to the next appropriate step in their care journey. This can be done by: appropriately trained non-clinical staff normally in the form of 'care navigation' care coordinators.
How do I say no to patient requests?
Saying no to these requests while preserving the patient relationship takes skill, but three tips can help. View the patient in the best possible light. This is the antidote to further deterioration of a difficult patient interaction. Explicitly state that the patient's request is inappropriate. Reestablish rapport.
What is a patient requisition?
Requisition forms, sometimes called referral forms, are used by your doctor or local physician to communicate precisely what type of exam you require for a medical assessment. These forms direct our technologists by outlining where diagnostic imaging is needed, such as your left shoulder or right ankle.
What is a request form in the hospital?
A patient request for medical records form is a document patients fill out to get copies of their medical information. It helps patients access their health records easily.
How do I say no to patient requests?
Saying no to these requests while preserving the patient relationship takes skill, but three tips can help. View the patient in the best possible light. This is the antidote to further deterioration of a difficult patient interaction. Explicitly state that the patient's request is inappropriate. Reestablish rapport.
What is a patient request?
It means a health care provider must: Allow a patient to inspect his or her record. Provide a copy or summary of the record if requested by the patient. Transmit a copy of the record to a person or entity of the patient's choosing. Requests for this type of access must be written.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is Patient Request Form?
A Patient Request Form is a document that allows patients to formally request access to their medical records or to authorize the release of their health information.
Who is required to file Patient Request Form?
Patients or their authorized representatives are required to file a Patient Request Form to obtain their medical records or to designate someone else to access their information.
How to fill out Patient Request Form?
To fill out a Patient Request Form, provide personal identification information, specify the records being requested, and indicate whether the request is for your own records or for another authorized individual.
What is the purpose of Patient Request Form?
The purpose of the Patient Request Form is to ensure patients have a clear and formal process to access their health information, maintain their privacy rights, and comply with health information regulations.
What information must be reported on Patient Request Form?
The Patient Request Form must typically report the patient's full name, date of birth, contact information, details of the information requested, and date of the request.
Fill out your patient request form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Patient Request Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
