Last updated on Apr 10, 2026
Get the free Providence Medicare Plan Selection Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is providence medicare plan selection
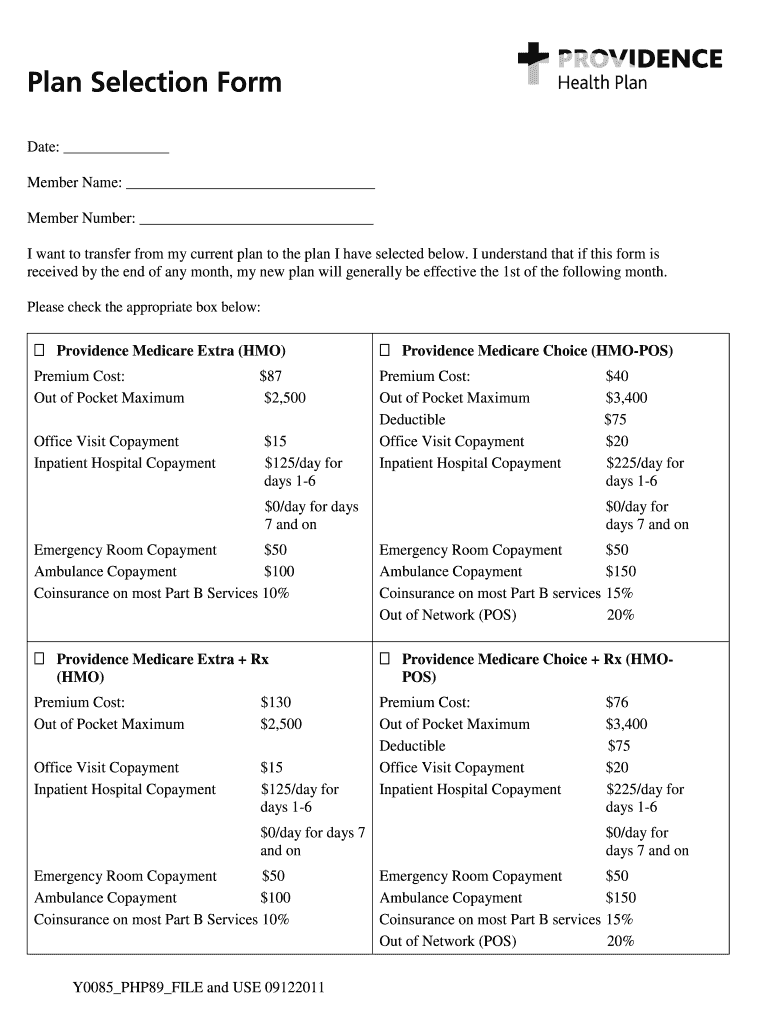
The Providence Medicare Plan Selection Form is a healthcare document used by members to transfer from their current Medicare plan to a new plan offered by Providence Medicare Advantage Plans.
pdfFiller scores top ratings on review platforms
Who needs providence medicare plan selection?
Explore how professionals across industries use pdfFiller.

Providence medicare plan selection is needed by:
-
Individuals enrolled in Medicare seeking a new plan
-
Authorized representatives assisting members in plan selection
-
Healthcare providers offering guidance on Medicare options
-
Insurance agents specializing in Medicare Advantage Plans
-
Family members supporting seniors in healthcare decisions
Comprehensive Guide to providence medicare plan selection
Overview of the Providence Medicare Plan Selection Form
The Providence Medicare Plan Selection Form is designed to facilitate the transition for members moving to a new Medicare plan endorsed by Providence. Its primary function is to streamline the process of plan selection and ensure that all necessary personal information is accurately captured. Completing this form is vital for members looking to transfer to a new Medicare plan, especially given the unique options available in Oregon.
When filling out the Providence Medicare Plan Selection Form, users must provide essential personal information and indicate their chosen plan. This organized approach helps maintain clarity and efficiency in managing Medicare options.
Purpose and Benefits of the Providence Medicare Plan Selection Form
This form serves as a crucial tool for members wishing to switch their Medicare plans. It simplifies the often complex process of plan transfer, ensuring that members can find a healthcare plan that aligns with their specific needs.
-
It enables users to easily choose a Medicare Advantage plan that fits their requirements.
-
Members enjoy increased options for premium payment selection and format preferences, enhancing overall satisfaction and service customization.
Who Should Use the Providence Medicare Plan Selection Form
The target audience for the Providence Medicare Plan Selection Form includes current Medicare beneficiaries and their authorized representatives. Understanding who must utilize this form ensures proper submission and adherence to guidelines.
-
Eligible members must fill out the form to initiate any necessary plan changes.
-
Authorized representatives can sign the form on behalf of members, provided they have appropriate consent.
-
Common scenarios requiring this form include changing health needs or relocating to a new area.
How to Fill Out the Providence Medicare Plan Selection Form Online
Completing the form online using pdfFiller is a straightforward process. Users can navigate through the fillable fields that prompt the entry of personal details and their selected Medicare plan.
-
Access the online form on pdfFiller.
-
Fill in designated sections with personal information and plan selection.
-
Review each section for accuracy to ensure that all information is complete before submission.
Essential Information Needed to Complete the Form
Before initiating the completion of the Providence Medicare Plan Selection Form, users should gather all necessary information and documentation. This preparation helps minimize errors and improves the efficiency of the process.
-
Required personal information includes full name, address, and date of birth.
-
Additional necessary documentation may consist of current Medicare card details and any previous plan information.
-
Members should also consider their premium payment options, selecting preferences that align with their financial situation.
Common Errors to Avoid While Filling the Form
To successfully navigate the completion of the Providence Medicare Plan Selection Form, users must be aware of common pitfalls that could lead to delays or rejections. Such awareness can help streamline the submission process.
-
Caution against overlooking key fields or providing incomplete information.
-
Double-check all provided data for accuracy, particularly in vital sections such as personal identification.
-
Ensure that the form is signed and dated appropriately to validate the submission.
Submitting the Providence Medicare Plan Selection Form
Proper submission of the Providence Medicare Plan Selection Form is essential for timely processing. Members should follow specific guidelines to ensure their application is handled efficiently.
-
Mail completed forms to the designated address in Portland, Oregon.
-
Familiarize yourself with any submission deadlines to avoid delays.
-
Keep a confirmation of sending to track the status of your application.
What Happens After Submission of the Form
Once the form is submitted, members can expect a series of notifications and must follow up appropriately to ensure progress on their applications. Understanding these steps can help manage expectations and outcomes.
-
Confirmation notifications may be issued following submission to verify receipt.
-
Members are advised on how to check the status of their application and any further follow-up procedures required.
-
Outcomes may vary, so it’s crucial to remain informed about potential approvals or rejections.
Security and Compliance for the Providence Medicare Plan Selection Form
Security is a vital consideration when handling sensitive information through the Providence Medicare Plan Selection Form. Users need to understand the protective measures in place to secure their data.
-
pdfFiller implements stringent security measures, ensuring HIPAA and GDPR compliance.
-
Maintaining confidentiality and securely managing personal information is a top priority.
-
Users can utilize secure eSigning options to safeguard their submissions further.
Ease of Completing the Providence Medicare Plan Selection Form with pdfFiller
The pdfFiller platform enhances the user experience during the completion of the Providence Medicare Plan Selection Form. Utilizing this tool can significantly simplify the process.
-
Benefits include customizable options for editing, signing, and sharing forms efficiently.
-
Features such as saving progress and easy access to completed forms support a smooth experience.
-
Members are encouraged to take advantage of pdfFiller's tools for a quick and secure completion process.
How to fill out the providence medicare plan selection
-
1.To access the Providence Medicare Plan Selection Form on pdfFiller, visit the pdfFiller website and use the search function to locate the form by its name.
-
2.Once the form is open, navigate through each section using the intuitive interface, ensuring that you are familiar with the layout and fields.
-
3.Before filling out the form, gather all necessary personal information such as your Medicare details, preferences for the new plan, and premium payment options.
-
4.Begin completing the form by entering your personal information in the designated fields such as name, address, and contact details.
-
5.As you move through the form, select your preferred Medicare plan in the 'Please check the appropriate box below:' section, ensuring it aligns with your needs.
-
6.Fill out any additional required fields, including your chosen premium payment option and any requests for information in different formats or languages.
-
7.After completing the form, carefully review all entered information for accuracy. Ensure that all required fields are filled appropriately and check for any mistakes.
-
8.Finalize the form by signing in the designated signature field, or ensuring that your authorized representative also signs if applicable.
-
9.Once finalized, use pdfFiller's options to save your completed form. Download a copy for your records and have the option to submit it via mail as indicated in the instructions.
-
10.To submit, print the form and mail it to the provided address in Portland, Oregon, ensuring all documents are correctly addressed.

Who is eligible to use the Providence Medicare Plan Selection Form?
Eligible users include individuals currently enrolled in Medicare who wish to change their plan. Authorized representatives can also complete the form on behalf of a member.
What is the deadline for submitting the Medicare Plan Selection Form?
Deadlines vary based on plan enrollment periods, usually aligning with Medicare's annual enrollment schedule. Check specific dates related to your insurance provider.
How can I submit the completed form?
The completed form must be mailed to the provided address in Portland, Oregon. Ensure you have signed it and included any necessary documents.
What documents do I need to support my application?
While specific supporting documents are generally not required, having your Medicare details and personal identification information handy is essential when filling out the form.
What common mistakes should I avoid when completing the form?
Ensure that all fields are accurately filled out without leaving blanks. Double-check signature requirements and read the entire form to avoid missing critical selections.
How long does processing of the form take?
Processing times can vary, but typically expect a response within a few weeks. Contact your Medicare plan provider for specific timelines.
What if I need assistance while filling out the form?
If you require help, consult with a family member or contact a representative from your Medicare plan. There are also various online resources available for guidance.
Related Forms



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.