Get the free Authorization for Medication - Luckiamute Valley Charter Schools - lvcs k12 or
Show details
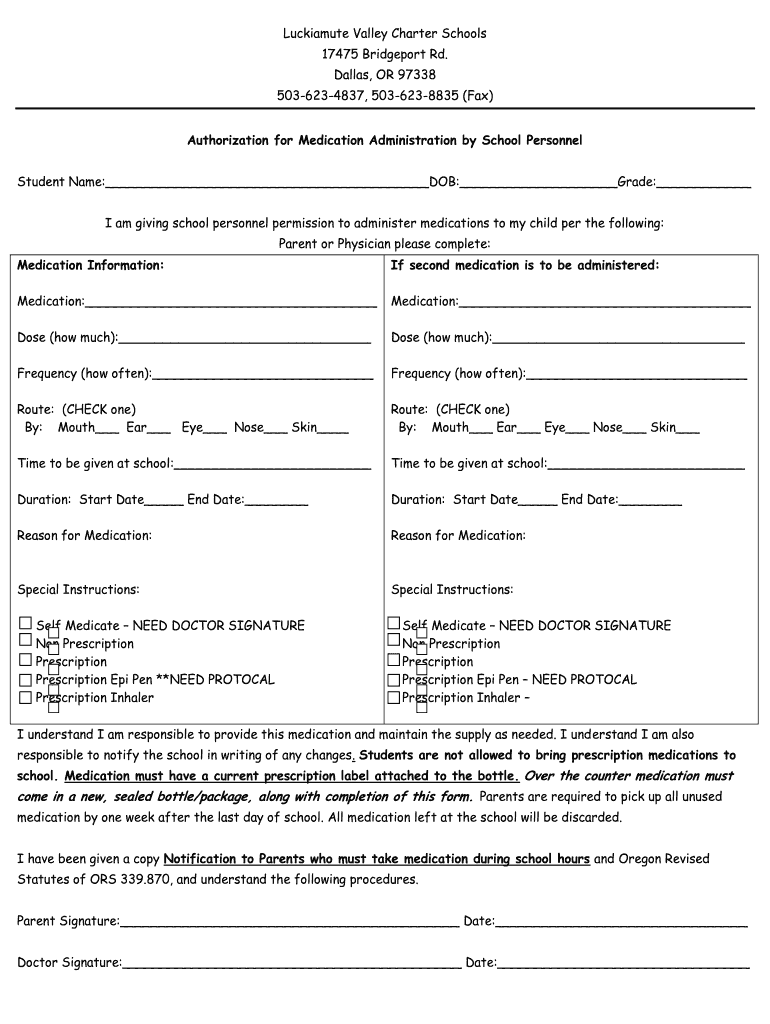
Luckiamute Valley Charter Schools 17475 Bridgeport Rd. Dallas, OR 97338 5036234837, 5036238835 (Fax) Authorization for Medication Administration by School Personnel Student Name: DOB: Grade: I am
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign authorization for medication

Edit your authorization for medication form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your authorization for medication form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing authorization for medication online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Log in to your account. Click Start Free Trial and sign up a profile if you don't have one yet.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit authorization for medication. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Save your file. Select it from your list of records. Then, move your cursor to the right toolbar and choose one of the exporting options. You can save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud, among other things.
pdfFiller makes dealing with documents a breeze. Create an account to find out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out authorization for medication

How to Fill Out Authorization for Medication:
01
Obtain the necessary form: Start by obtaining the specific authorization form for medication. This form is typically provided by the healthcare provider, pharmacy, or insurance company. You can request the form directly, download it from the provider's website, or visit the nearest pharmacy or medical office.
02
Read and understand the instructions: Carefully read through the instructions provided on the authorization form. Understand the purpose of the form, what information is required, and any specific guidelines or restrictions mentioned. This will help ensure you fill out the form correctly.
03
Fill in personal information: Begin by filling in your personal information accurately. This may include your full name, address, phone number, date of birth, and social security number. Double-check the information to avoid any mistakes that could delay authorization.
04
Provide healthcare provider information: Next, provide the information of your healthcare provider who prescribed the medication. This typically includes their name, clinic or practice name, address, phone number, and any relevant identification numbers (such as their National Provider Identifier).
05
Specify the medication details: Fill in the details of the medication being authorized. This may involve writing down the medication name, strength, dosage instructions, and the reason for its use. If you have the prescription label or the medication package, refer to it for accurate information.
06
Indicate the duration and quantity: Specify the duration for which the medication authorization is needed. This could be the number of days, weeks, or months. Additionally, mention the quantity of medication required, such as the number of pills or the volume of liquid in milliliters.
07
Include any additional information: If there are any additional details required, such as any allergies or special instructions, provide them in the designated sections. This information can help ensure safe and appropriate use of the medication.
08
Sign and date the form: Once all the necessary information has been filled in, sign and date the authorization form. This verifies that the information provided is accurate and that you authorize the release of the specified medication.
Who Needs Authorization for Medication?
01
Patients requiring certain controlled substances: Authorization for medication is often required for individuals who need specific controlled substances, such as opioids or certain psychiatric medications. This helps regulate their use and prevent misuse.
02
Insurance plan coverage: Some insurance plans require authorization for certain medications before they will provide coverage. This ensures that the prescribed medication is medically necessary and aligns with the insurance plan's formulary.
03
Prescription refills beyond a certain limit: In some cases, authorization may be necessary for prescription refills beyond a certain limit. This helps prevent excessive or unnecessary medication use and enables healthcare providers to reassess the patient's condition periodically.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
Can I sign the authorization for medication electronically in Chrome?
You can. With pdfFiller, you get a strong e-signature solution built right into your Chrome browser. Using our addon, you may produce a legally enforceable eSignature by typing, sketching, or photographing it. Choose your preferred method and eSign in minutes.
Can I create an eSignature for the authorization for medication in Gmail?
Create your eSignature using pdfFiller and then eSign your authorization for medication immediately from your email with pdfFiller's Gmail add-on. To keep your signatures and signed papers, you must create an account.
How do I fill out authorization for medication on an Android device?
On an Android device, use the pdfFiller mobile app to finish your authorization for medication. The program allows you to execute all necessary document management operations, such as adding, editing, and removing text, signing, annotating, and more. You only need a smartphone and an internet connection.
What is authorization for medication?
Authorization for medication is the process of obtaining permission to administer or receive a specific medication.
Who is required to file authorization for medication?
Healthcare providers, pharmacies, and individuals may be required to file authorization for medication depending on the specific circumstances.
How to fill out authorization for medication?
Authorization for medication typically involves providing information about the patient, the medication being prescribed, the dosage and frequency, and the prescribing healthcare provider.
What is the purpose of authorization for medication?
The purpose of authorization for medication is to ensure that the appropriate medication is prescribed to the right patient in the correct dosage and frequency.
What information must be reported on authorization for medication?
Information such as patient demographics, medication name, dosage, frequency, prescribing healthcare provider, and any relevant medical conditions or allergies must be reported on authorization for medication.
Fill out your authorization for medication online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Authorization For Medication is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
