
Get the free PROVIDER ENROLLMENT FORM FOR WPS-Medicare Part B MN
Show details
EAC Submissions 5705 Fieldstone Try. McHenry, IL 60050 8155784122 pH. 8153854022 fax www.easyambulanceclaims.com PROVIDER ENROLLMENT FORM FOR: WPS Medicare Part B (MN) INSTRUCTIONS: Complete and sign
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign provider enrollment form for
Edit your provider enrollment form for form online
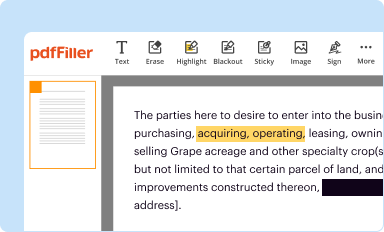
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
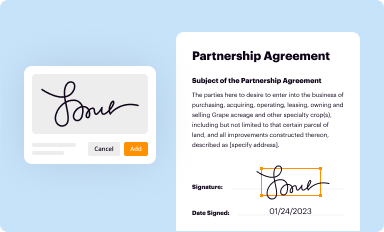
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
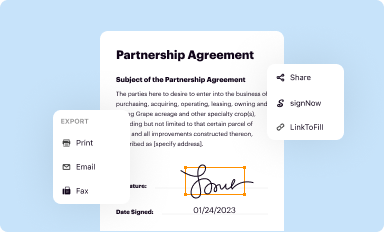
Share your form instantly
Email, fax, or share your provider enrollment form for form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit provider enrollment form for online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit provider enrollment form for. Rearrange and rotate pages, insert new and alter existing texts, add new objects, and take advantage of other helpful tools. Click Done to apply changes and return to your Dashboard. Go to the Documents tab to access merging, splitting, locking, or unlocking functions.
4
Get your file. Select the name of your file in the docs list and choose your preferred exporting method. You can download it as a PDF, save it in another format, send it by email, or transfer it to the cloud.
pdfFiller makes working with documents easier than you could ever imagine. Register for an account and see for yourself!
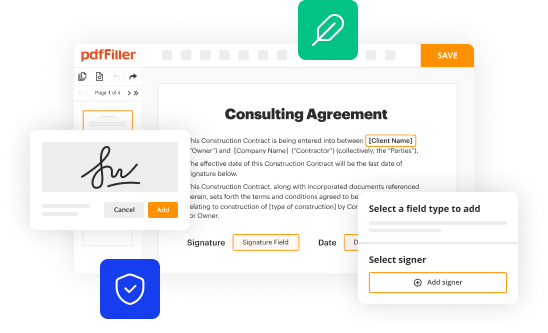
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out provider enrollment form for
How to fill out provider enrollment form for:
01
Gather all necessary documents and information: Before starting the form, make sure you have all the required documents and information handy. This may include your personal identification, proof of education or certification, professional license, and any other relevant documents.
02
Read the instructions carefully: Provider enrollment forms can vary based on the specific organization or agency. Take the time to carefully read through the instructions provided with the form. This will ensure you understand the requirements and provide the correct information.
03
Provide accurate personal information: Start by filling out your personal information accurately. This may include your full name, address, contact details, and social security number. Ensure you double-check this information for any errors or typos.
04
Fill out your professional details: Provide detailed information about your professional background. This may include your education, certifications, licenses, specializations, and prior experience. Be sure to include any relevant dates, such as graduation or certification dates.
05
Include your billing and payment information: If applicable, you may need to provide billing and payment details. This can include your tax identification number, bank account information, or any other relevant payment details. Ensure you provide accurate and up-to-date information.
06
Provide any additional requested information: Depending on the specific form, there may be additional sections or questions that need to be addressed. Take the time to carefully read and respond to each section accordingly. This may include questions about malpractice insurance, affiliations, or professional references.
Who needs provider enrollment form for:
01
Healthcare professionals: Healthcare professionals, such as physicians, nurses, dentists, therapists, and other healthcare practitioners, may need to fill out provider enrollment forms. This is often required to become an approved provider for insurance companies, Medicare, Medicaid, or other healthcare programs.
02
Medical facilities: Hospitals, clinics, nursing homes, and other healthcare facilities may also need to complete provider enrollment forms. This allows them to bill insurance companies or government programs for the services provided by their healthcare practitioners.
03
Allied healthcare providers: Allied healthcare providers, including medical billing companies, medical equipment suppliers, and home healthcare agencies, may also require provider enrollment forms. This ensures they can provide their services and receive payment from insurance companies or government programs.
Overall, provider enrollment forms are necessary for individuals and organizations looking to become approved providers within the healthcare industry. The forms help establish a formal relationship with insurance companies, government programs, and other entities involved in healthcare reimbursement.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I make edits in provider enrollment form for without leaving Chrome?
Install the pdfFiller Chrome Extension to modify, fill out, and eSign your provider enrollment form for, which you can access right from a Google search page. Fillable documents without leaving Chrome on any internet-connected device.
How do I edit provider enrollment form for straight from my smartphone?
Using pdfFiller's mobile-native applications for iOS and Android is the simplest method to edit documents on a mobile device. You may get them from the Apple App Store and Google Play, respectively. More information on the apps may be found here. Install the program and log in to begin editing provider enrollment form for.
How do I edit provider enrollment form for on an Android device?
You can edit, sign, and distribute provider enrollment form for on your mobile device from anywhere using the pdfFiller mobile app for Android; all you need is an internet connection. Download the app and begin streamlining your document workflow from anywhere.
What is provider enrollment form for?
The provider enrollment form is used to enroll healthcare providers in insurance networks.
Who is required to file provider enrollment form for?
Healthcare providers are required to file provider enrollment form to be part of insurance networks.
How to fill out provider enrollment form for?
Provider enrollment form can be filled out online or by submitting a paper application with required documentation.
What is the purpose of provider enrollment form for?
The purpose of provider enrollment form is to ensure that healthcare providers meet the guidelines and standards set by insurance networks.
What information must be reported on provider enrollment form for?
Provider enrollment form requires information such as provider's credentials, contact information, practice location, and specialty.
Fill out your provider enrollment form for online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Provider Enrollment Form For is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
