
Get the free Provider Nomination Form
Show details
This document is used to nominate a dentist to join a provider network, including details about the patient and the dentist.
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign provider nomination form
Edit your provider nomination form form online
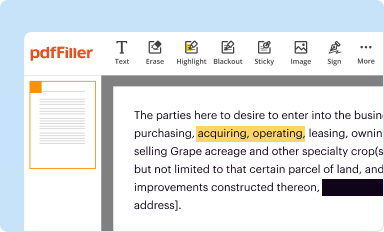
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
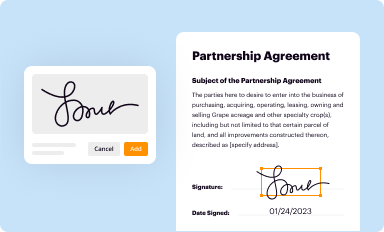
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
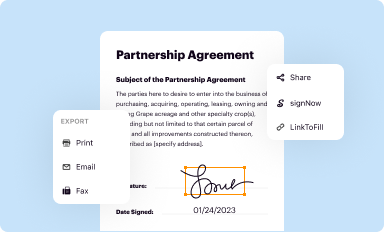
Share your form instantly
Email, fax, or share your provider nomination form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit provider nomination form online



Follow the steps down below to benefit from a competent PDF editor:
1
Register the account. Begin by clicking Start Free Trial and create a profile if you are a new user.
2
Upload a file. Select Add New on your Dashboard and upload a file from your device or import it from the cloud, online, or internal mail. Then click Edit.
3
Edit provider nomination form. Add and replace text, insert new objects, rearrange pages, add watermarks and page numbers, and more. Click Done when you are finished editing and go to the Documents tab to merge, split, lock or unlock the file.
4
Get your file. When you find your file in the docs list, click on its name and choose how you want to save it. To get the PDF, you can save it, send an email with it, or move it to the cloud.
With pdfFiller, it's always easy to deal with documents.
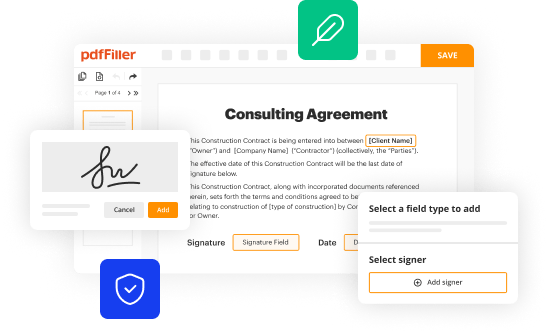
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out provider nomination form
How to fill out Provider Nomination Form
01
Obtain the Provider Nomination Form from the appropriate authority or website.
02
Fill in your personal details including name, contact information, and relevant identification.
03
Provide the details of the provider you are nominating, including their name, qualifications, and registry number.
04
Explain your relationship to the provider and the reasons for your nomination.
05
Ensure all information is accurate and complete before submission.
06
Review the form for any errors or omissions.
07
Submit the form as instructed, either electronically or by mailing it to the designated office.
Who needs Provider Nomination Form?
01
Health professionals who wish to nominate a provider for recognition.
02
Organizations seeking to endorse a provider for accreditation.
03
Individuals participating in programs or services that require provider nominations.
Fill
form
: Try Risk Free
People Also Ask about
What is a nomination form used for?
Nomination is part of the process of selecting a candidate for either election to a public office, or the bestowing of an honor or award. A collection of nominees narrowed from the full list of candidates is a short list.
How do I create a nomination form?
An award nomination form should include fields to collect the nominee's personal information, achievements, qualifications, supporting documents, and any additional information deemed relevant for the selection process. It should also include a section for the nominator's details and their rationale for the nomination.
What is the phone number for multiplan credentialing?
For questions about our credentialing process or joining our networks, call our Service Operations Department at 1-800-950-7040.
Are PHCS and MultiPlan the same?
Please provide a detailed description of the service being provided and the code to a member of our Customer Care Team at 1-800-869-7093 and they will provide you with an accurate benefit quote. Where should I submit claims?
How do I contact MultiPlan credentialing?
For questions about our credentialing process or joining our networks, call our Service Operations Department at 1-800-950-7040.
What is the phone number for MultiPlan PHCS?
2. Always verify a provider's participation in the PHCS network before obtaining services. If a PHCS provider refers you to another provider, participation for that provider should also be confirmed before obtaining services. To do this, call 844-863-6850 or call MultiPlan at 800-922-4362.
What do you write in a nomination form?
Describe specific characteristics, qualities, or examples that you believe make the nominee stand out or demonstrate how they go above and beyond. Quality is appreciated more than quantity. A well-written and concise submission increases the likelihood of a positive outcome. Use an active voice in your writing.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is Provider Nomination Form?
The Provider Nomination Form is a document used to designate a specific service provider for particular medical, healthcare, or insurance needs within a health network.
Who is required to file Provider Nomination Form?
Typically, patients, members of health plans, or healthcare organizations seeking to nominate a provider for inclusion in their care network are required to file the Provider Nomination Form.
How to fill out Provider Nomination Form?
To fill out the Provider Nomination Form, individuals must provide necessary details such as personal information, the provider’s information, and any relevant documentation to support the nomination.
What is the purpose of Provider Nomination Form?
The purpose of the Provider Nomination Form is to facilitate the process of adding or recommending healthcare providers to a network, ensuring that patients can access needed services more effectively.
What information must be reported on Provider Nomination Form?
The information that must be reported on the Provider Nomination Form typically includes the nominee's name, contact information, specialty, reason for nomination, and any supporting evidence of qualifications.
Fill out your provider nomination form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Provider Nomination Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
