
Get the free Member Self-Pay Reimbursement Form
Show details
This form is to be used for submitting claims for reimbursement of prescription expenses incurred when a participating pharmacy could not honor the identification card or was unable to submit the
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign member self-pay reimbursement form
Edit your member self-pay reimbursement form form online
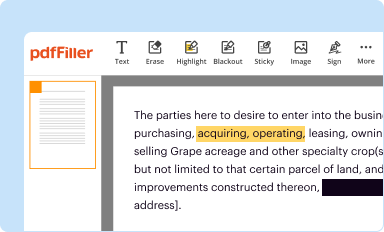
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
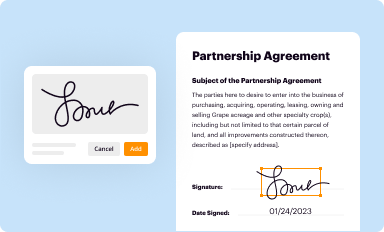
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
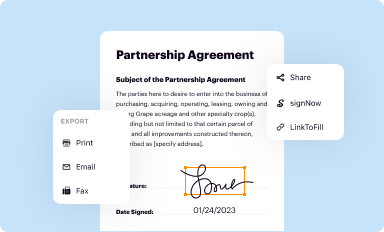
Share your form instantly
Email, fax, or share your member self-pay reimbursement form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing member self-pay reimbursement form online



In order to make advantage of the professional PDF editor, follow these steps below:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Upload a file. Select Add New on your Dashboard and upload a file from your device or import it from the cloud, online, or internal mail. Then click Edit.
3
Edit member self-pay reimbursement form. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
With pdfFiller, it's always easy to deal with documents.
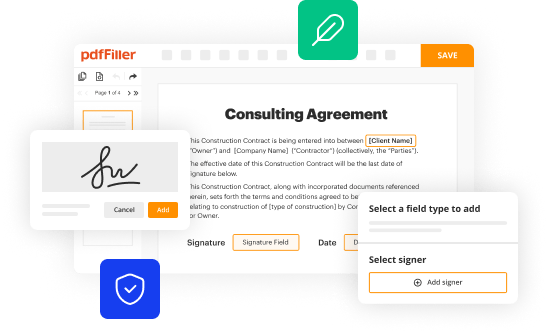
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out member self-pay reimbursement form
How to fill out Member Self-Pay Reimbursement Form
01
Obtain the Member Self-Pay Reimbursement Form from the appropriate source such as the health plan's website or member services.
02
Fill in your personal information at the top of the form, including your name, member ID, and contact information.
03
Provide details about the medical expenses you are claiming reimbursement for, including the date of service, provider name, and amount paid.
04
Attach all relevant receipts and documentation that support your claim for reimbursement.
05
Review the form for accuracy and completeness before signing it.
06
Submit the completed form along with the attached documents to the specified address or email provided by your health plan.
Who needs Member Self-Pay Reimbursement Form?
01
Members who have paid for medical services out-of-pocket and wish to seek reimbursement from their health insurance plan.
Fill
form
: Try Risk Free
People Also Ask about
How to fill out an expense reimbursement form?
For the business to verify that the expense was actually work-related, it's important to include all essential information about the expense on your reimbursement form: Name of product or service. Individual item or line cost. Total cost. Payment method (i.e., cash, credit card, etc.) Date purchased. Explanation of purchase.
What is a direct member reimbursement form?
A Direct Member Reimbursement (DMR) is when you ask us to pay you back for prescription drugs you paid for out-of-pocket.
How do I fill out a reimbursement claim form?
Follow the steps given below to file a reimbursement health insurance claim: Step 1: Inform the Insurance Company. Step 2: Obtain Treatment. Step 3: Pay the Hospital Bill. Step 4: Collect All Your Documents. Step 5: Fill up the Claim Form. Step 6: Submit All Documents to the Insurance Company.
How do I write a reimbursement claim?
Step-by-Step: How to Write an Insurance Claim Letter for Reimbursement Begin with Your Contact Details and Date. Address the Letter Appropriately. State the Purpose Clearly with a Subject Line. Introduce Yourself and Reference Your Policy. Describe the Incident or Expense in Detail.
How to fill a reimbursement form?
How to Fill Care Health Insurance Claim Reimbursement Form Step 1: Fill Out the Details of the Primary Insured. Step 2: Disclose the Insurance History of the Person Filing Claim. Step 3: List Down the Details of the Insured Person Hospitalized. Step 4: Enter the Hospitalization Information.
How do I process a reimbursement claim?
Here is the process, categorised into different steps for a clearer understanding: Intimate the insurance company. Pay bills and collect documents. Submit the claim form and documents. Let the insurance company verify and enquire.
How to submit for reimbursement with UnitedHealthcare?
There are 2 ways to submit claims — online or by mail You will have the option to digitally submit a form or download, print and mail a medical claim form (pdf) to the mailing address found on your member ID card.
How to fill a NAS reimbursement form?
The NAS reimbursement claim form must include the insured's name, card number, diagnosis, and details of medical services rendered. Use a separate NAS claim form for each insured member. The reimbursement procedure usually takes 15 working days from the date of successful document upload.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is Member Self-Pay Reimbursement Form?
The Member Self-Pay Reimbursement Form is a document used by members to request reimbursement for medical expenses that they have paid out of pocket, typically for services that are covered by their insurance plan.
Who is required to file Member Self-Pay Reimbursement Form?
Members who have paid for medical services themselves and wish to seek reimbursement from their insurance provider are required to file the Member Self-Pay Reimbursement Form.
How to fill out Member Self-Pay Reimbursement Form?
To fill out the form, members must provide their personal details, including name and insurance information, detail the services received, attach payment receipts, and sign the form to confirm the accuracy of the information provided.
What is the purpose of Member Self-Pay Reimbursement Form?
The purpose of the Member Self-Pay Reimbursement Form is to facilitate the process for members to receive reimbursement for eligible medical expenses that they have already paid out of their own pockets.
What information must be reported on Member Self-Pay Reimbursement Form?
The information that must be reported includes the member's name, policy number, date of service, type of service received, amount paid, and submission of relevant receipts and documentation to support the reimbursement request.
Fill out your member self-pay reimbursement form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Member Self-Pay Reimbursement Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
