Get the free DALIRESP™ (ROFLUMILAST) PHYSICIAN FAX FORM
Show details
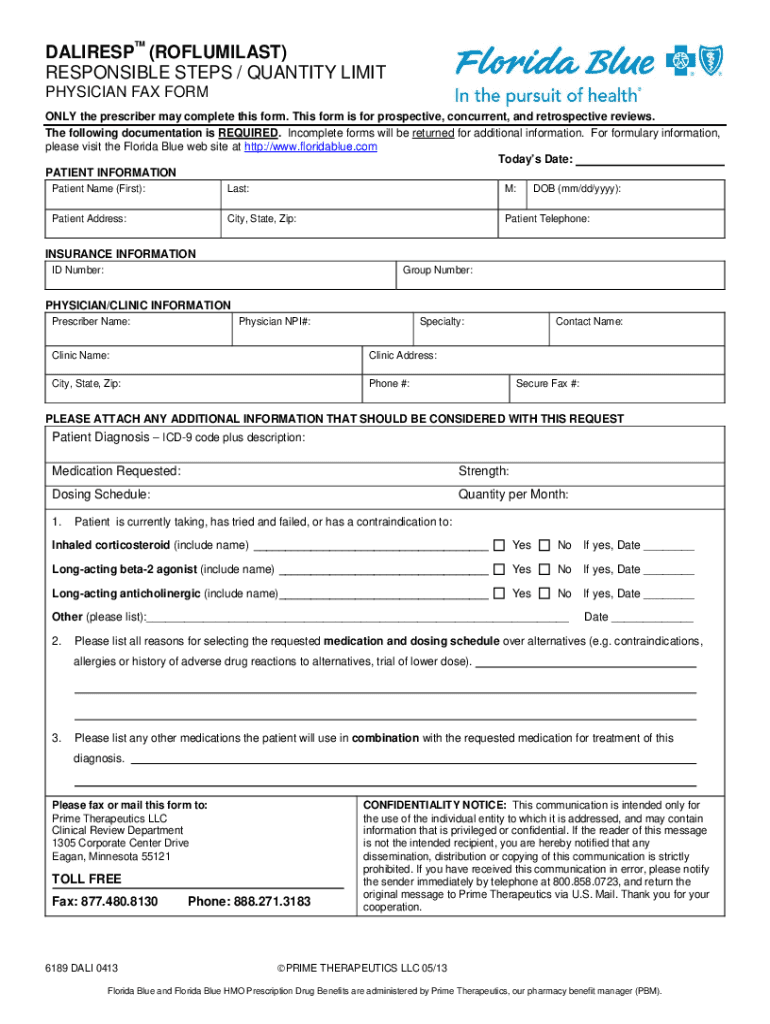
This form is intended for physicians to complete in order to request prior authorization for the medication DALIRESP™. It includes sections for patient and physician information, medication details,
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign daliresp roflumilast physician fax
Edit your daliresp roflumilast physician fax form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your daliresp roflumilast physician fax form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit daliresp roflumilast physician fax online



To use our professional PDF editor, follow these steps:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit daliresp roflumilast physician fax. Add and replace text, insert new objects, rearrange pages, add watermarks and page numbers, and more. Click Done when you are finished editing and go to the Documents tab to merge, split, lock or unlock the file.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
With pdfFiller, it's always easy to work with documents. Try it out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out daliresp roflumilast physician fax
How to fill out DALIRESP™ (ROFLUMILAST) PHYSICIAN FAX FORM
01
Obtain the DALIRESP™ (ROFLUMILAST) PHYSICIAN FAX FORM from a reliable source.
02
Fill in the patient’s personal information including name, date of birth, and contact details.
03
Provide the physician's information including name, address, and phone number.
04
Complete the medical history section, detailing relevant diagnoses and treatments.
05
Specify the prescribed dosage and any other relevant treatment notes.
06
Sign and date the form to verify it is complete.
07
Ensure all sections of the form are filled out clearly and legibly.
08
Submit the completed form via fax to the appropriate recipient as indicated on the form.
Who needs DALIRESP™ (ROFLUMILAST) PHYSICIAN FAX FORM?
01
Physicians prescribing DALIRESP™ (ROFLUMILAST) to their patients.
02
Medical staff responsible for coordinating treatment for patients with COPD.
03
Patients whose treatment requires physician approval for medication initiation.
Fill
form
: Try Risk Free
People Also Ask about
Does affect the kidneys?
Serious adverse reactions, whether considered drug-related or not by the investigators, which occurred more frequently in -treated patients include diarrhea, atrial fibrillation, lung cancer, prostate cancer, acute pancreatitis, and acute renal failure.
What does do for the lungs?
Roflumilast () is a phosphodiesterase-4 (PDE-4) inhibitor. It blocks PDE-4, a protein in your body that's involved in causing inflammation in the lungs and making it difficult for you to breathe. By blocking PDE-4, roflumilast () lessens inflammation and opens up your airways to help you breathe better.
Is the same as roflumilast?
Roflumilast (): A Novel Phosphodiesterase-4 Inhibitor for the Treatment Of Severe Chronic Obstructive Pulmonary Disease - PMC.
What are the most common side effects of ?
Diarrhea and nausea were the two side effects that most often caused people to discontinue treatment with in clinical trials. In these clinical trials, most of the people who had diarrhea and/or nausea experienced it in the beginning of their treatment, and it generally lasted less than four weeks.
How much does cost?
Roflumilast () dosage forms The average cost for 30 tablets of 500mcg of Roflumilast () is $456.32 with a free GoodRx coupon. This is 15.18% off the average retail price of $537.95.
Is an anti-inflammatory?
Other drugs are generally used as adjunctive or second-line agents. One adjunctive agent, roflumilast (, Forest), is the first new therapy for COPD in nearly 20 years. Early clinical trials sought to obtain indications for roflumilast in asthma and allergic rhinitis because of its anti-inflammatory properties.
What is the medicine used for?
is a prescription medicine used in adults with severe Chronic Obstructive Pulmonary Disease (COPD) to decrease the number of flare-ups or the worsening of COPD symptoms (exacerbations). is not a bronchodilator and should not be used for treating sudden breathing problems.
Is good for COPD?
The medication –the first and only medicine of its kind for COPD–may help to decrease the risk of future flare-ups in adults with severe COPD.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is DALIRESP™ (ROFLUMILAST) PHYSICIAN FAX FORM?
The DALIRESP™ (ROFLUMILAST) PHYSICIAN FAX FORM is a document used by healthcare providers to request authorization for the prescription of DALIRESP™, a medication indicated for the treatment of chronic obstructive pulmonary disease (COPD).
Who is required to file DALIRESP™ (ROFLUMILAST) PHYSICIAN FAX FORM?
Healthcare providers, such as physicians or nurse practitioners, who wish to prescribe DALIRESP™ for their patients are required to file the DALIRESP™ PHYSICIAN FAX FORM.
How to fill out DALIRESP™ (ROFLUMILAST) PHYSICIAN FAX FORM?
To fill out the DALIRESP™ PHYSICIAN FAX FORM, the healthcare provider should provide necessary patient information, including the patient's name, date of birth, insurance details, diagnosis, and medical history related to COPD. The form must be signed by the provider and sent to the appropriate insurance company or pharmacy.
What is the purpose of DALIRESP™ (ROFLUMILAST) PHYSICIAN FAX FORM?
The purpose of the DALIRESP™ PHYSICIAN FAX FORM is to facilitate the approval process for the prescription of DALIRESP™, ensuring that patients receive the necessary medication to manage their condition effectively.
What information must be reported on DALIRESP™ (ROFLUMILAST) PHYSICIAN FAX FORM?
The DALIRESP™ PHYSICIAN FAX FORM must report patient demographics, insurance information, relevant medical history, diagnosis of COPD, current medications, and any other details required by the insurance provider to process the prescription authorization.
Fill out your daliresp roflumilast physician fax online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Daliresp Roflumilast Physician Fax is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
