Last updated on May 20, 2026
CHCB Dental Patient Medical History Form 2013-2026 free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
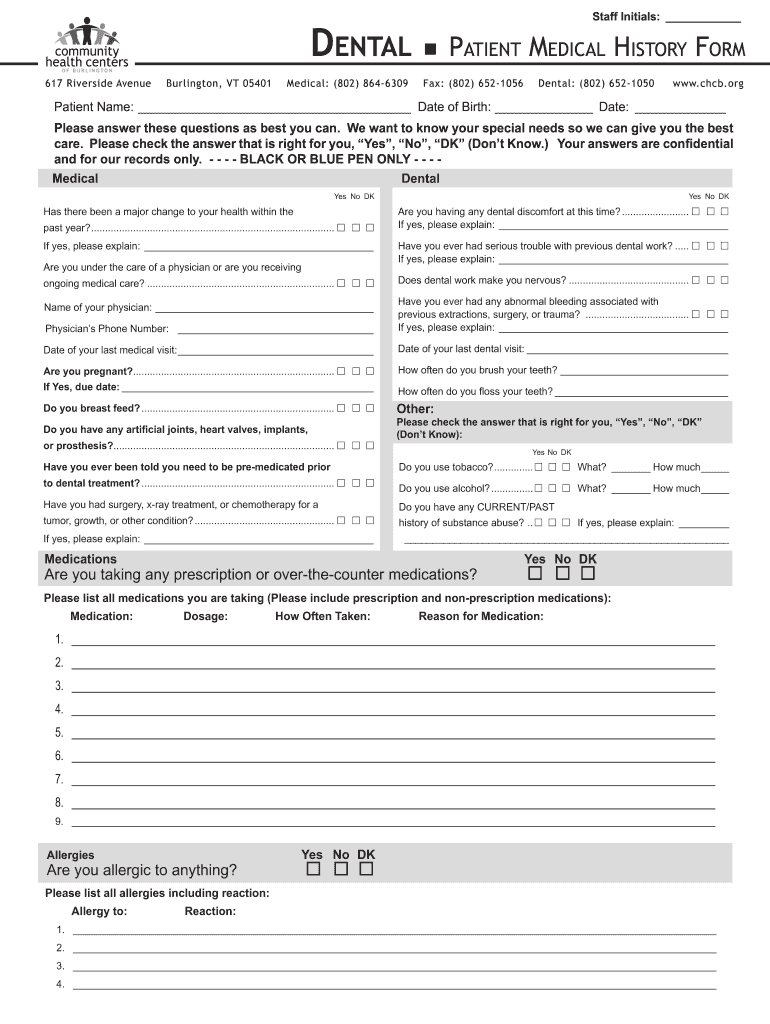
What is CHCB Dental Patient Medical History Form
The Dental Patient Medical History Form is a medical document used by dental clinics to collect comprehensive medical and dental history information from patients.
pdfFiller scores top ratings on review platforms
Who needs CHCB Dental Patient Medical History Form?
Explore how professionals across industries use pdfFiller.

CHCB Dental Patient Medical History Form is needed by:
-
Patients seeking dental care.
-
Guardians completing forms for minor patients.
-
Dental hygienists requiring patient information.
-
Dentists reviewing patient history.
-
Dental administrative staff processing intake forms.
Comprehensive Guide to CHCB Dental Patient Medical History Form
What is the Dental Patient Medical History Form?
The Dental Patient Medical History Form is a vital tool used in dental care to gather extensive medical and dental histories from patients. This form plays a crucial role in ensuring that healthcare providers can offer personalized care based on individual health backgrounds.
This form typically includes personal details such as name and date of birth, as well as important medical information like existing conditions and medications. By collecting this data, dental professionals can gain insights into any health concerns that may impact treatment.
Purpose and Benefits of Completing the Dental Patient Medical History Form
Completing the dental health questionnaire is essential for both patients and dental professionals. It enables healthcare providers to deliver optimal care by understanding a patient’s medical history thoroughly.
This form helps identify potential health issues that could affect dental procedures, fostering communication between the patient and the dental team. By detailing their medical backgrounds, patients ensure that they receive safe and effective dental care tailored to their specific needs.
Key Features of the Dental Patient Medical History Form
The dental patient medical history form is designed with user-friendliness in mind. It is organized into intuitive sections that include:
-
Personal information
-
Medical conditions
-
Medications
-
Allergies
This fillable form features checkboxes and blank fields, making it easy for patients to provide the necessary information. Additionally, it requires signatures from the patient or guardian, as well as from both the hygienist and the dentist, to ensure all parties are informed.
Who Should Complete the Dental Patient Medical History Form?
The responsibility of filling out the patient intake form dental falls on patients, guardians, and dental professionals. It is particularly important for guardians to fill out the form accurately for children, as accurate information is crucial for their dental care.
New patients must complete this form to establish a comprehensive profile, while returning patients should update their information to reflect any changes in their health status. This ensures that dental teams have the most current information to provide the best care possible.
How to Fill Out the Dental Patient Medical History Form Online (Step-by-Step)
Filling out the dental patient medical history form online is straightforward. Follow these steps:
-
Access the form through a reliable platform like pdfFiller.
-
Begin by entering your personal information in the designated fields.
-
Proceed to list any medical conditions or medications you are currently taking.
-
Provide details about any allergies and dental concerns.
-
Review your information for completeness before submission.
For accuracy, double-check all sections to prevent omitting critical details.
Common Errors and How to Avoid Them When Completing the Form
To ensure a smooth process, avoid common pitfalls when filling out the medical history form template:
-
Omitting required fields can delay your treatment.
-
Providing inaccurate information can lead to improper care.
-
Illegible handwriting may cause misunderstandings.
Reviewing the completed form carefully can help catch errors, ensuring clarity in responses and contributing to safer dental practices.
How to Submit the Dental Patient Medical History Form
Submitting the dental patient medical history form can be done through various convenient methods. You can choose to:
-
Submit the form online via a secure platform.
-
Print and submit the form in person at your dental practice.
-
Ensure you meet any deadlines set by your dental office to avoid delays.
After submission, expect a confirmation of receipt, which provides peace of mind that your information has been successfully processed.
Security and Compliance of the Dental Patient Medical History Form
Maintaining security and compliance of the dental patient medical history form is critical, especially regarding sensitive health information. The form adheres to HIPAA guidelines, ensuring that patient data remains protected through strong security measures, including encryption.
Patients should feel assured about their privacy when submitting personal health information. It is advisable to use reputable services, such as pdfFiller, for managing forms securely.
Why Use pdfFiller for Your Dental Patient Medical History Form?
pdfFiller stands out as the ideal platform for creating and managing the dental patient medical history form. Some benefits include:
-
Easy editing capabilities that simplify the completion of the form.
-
User-friendly interface that guides you through the process.
-
Robust eSigning and security features that ensure your information is safe.
By leveraging pdfFiller, you can enjoy a seamless experience while maintaining the integrity of your sensitive health data.
Get Started with Your Dental Patient Medical History Form Today!
Start your journey by accessing the online dental patient medical history form via pdfFiller. The process is designed to be easy, secure, and efficient, allowing you to take control of your dental health. Provide your accurate medical history today to ensure the best care possible.
How to fill out the CHCB Dental Patient Medical History Form
-
1.To access the Dental Patient Medical History Form on pdfFiller, navigate to the platform's search bar and enter the form name.
-
2.After finding the form, click on its title to open it in the pdfFiller editor, where you can fill it out online.
-
3.Before you start completing the form, gather essential information such as personal details, medical conditions, allergies, and current medications.
-
4.Using the pdfFiller interface, click on each blank field to input your information. Utilize the provided checkboxes where applicable, and follow the instructions for each section carefully.
-
5.Take your time to fill in all sections, ensuring you provide accurate information about your medical and dental history.
-
6.Once you have completed the form, carefully review all your entries for accuracy and completeness to avoid common mistakes.
-
7.To finalize the form, utilize pdfFiller's options to save your progress or submit the form directly to your dental clinic.

Who is required to sign the Dental Patient Medical History Form?
The Dental Patient Medical History Form requires signatures from the patient or guardian, the hygienist, and the dentist to ensure all parties acknowledge the provided medical information.
What information do I need to complete this form?
Before filling out the form, gather personal details like your name, date of birth, medical conditions, medications, and any known allergies to ensure accurate completion.
How can I submit the completed form?
Once you complete the Dental Patient Medical History Form, you can submit it directly through pdfFiller. Alternatively, you can download the file and email it to your dental clinic.
Are there specific deadlines for submitting this form?
It is best to submit the Dental Patient Medical History Form prior to your scheduled appointment. Check with your dental clinic for any specific deadlines they may have.
What should I do if I make a mistake on the form?
If you make a mistake while completing the form, you can easily edit any section within the pdfFiller interface. Make sure to review the entire form before finalizing it.
Is this form available in languages other than English?
The Dental Patient Medical History Form is currently available only in English. Consult your dental clinic for assistance with translations, if required.
Do I need to notarize this form?
No, the Dental Patient Medical History Form does not require notarization. Just ensure all necessary signatures are obtained.
Related Forms







Related Catalogs
Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.