Get the free as my physician, - sw
Show details
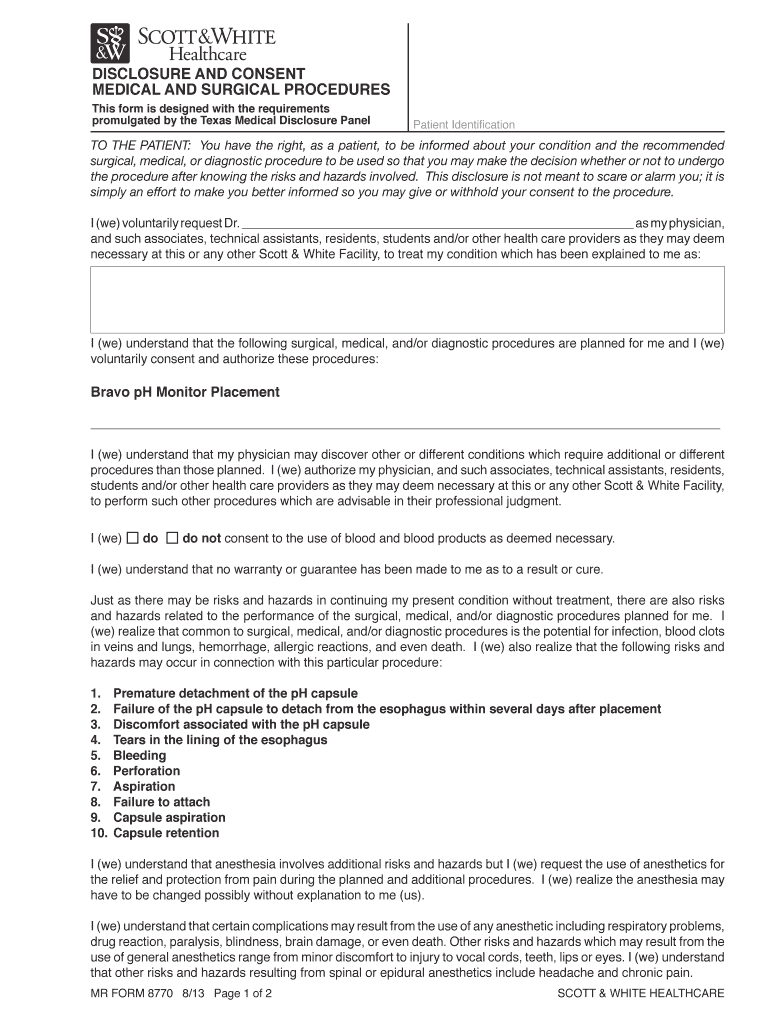
Management (Analgesia) consent form must also be reviewed and signed by anesthesia provider (i.e., anesthesiologist, CRNA, or operating practitioner who ...
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign as my physician
Edit your as my physician form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your as my physician form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing as my physician online



In order to make advantage of the professional PDF editor, follow these steps:
1
Log in to your account. Click on Start Free Trial and register a profile if you don't have one.
2
Upload a file. Select Add New on your Dashboard and upload a file from your device or import it from the cloud, online, or internal mail. Then click Edit.
3
Edit as my physician. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
With pdfFiller, it's always easy to work with documents.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out as my physician
How to fill out as my physician:
01
Gather all necessary documents and forms required to apply as a physician.
02
Provide accurate personal information such as your full name, contact information, and social security number.
03
Include details about your medical education and training, including the name of the medical school you attended, dates of attendance, and any specialties you have.
04
List all previous work experiences and positions held in the medical field, including internships, residencies, and fellowships.
05
Provide information about any certifications or licenses you hold, along with their expiration dates and issuing authorities.
06
Include any publications, research projects, or academic achievements relevant to your medical career.
07
Attach any supporting documents, such as letters of recommendation, transcripts, or proof of continuing medical education.
08
Review the application thoroughly for any errors or missing information before submitting it.
Who needs as my physician:
01
Individuals who require primary medical care and ongoing healthcare management.
02
Patients with chronic conditions or complex medical needs that require personalized care.
03
People seeking preventive care and health maintenance.
04
Individuals in need of specialist referrals or coordination of care between healthcare providers.
05
Patients seeking advice, diagnosis, and treatment of acute illnesses or injuries.
06
Those in need of medical documentation, such as work or school physicals, disability evaluations, or assistance for legal purposes.
07
Individuals who want to establish a long-term relationship with a healthcare provider for their overall well-being.
08
Patients seeking support and guidance in managing their overall health, lifestyle changes, and disease prevention.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I send as my physician to be eSigned by others?
Once your as my physician is ready, you can securely share it with recipients and collect eSignatures in a few clicks with pdfFiller. You can send a PDF by email, text message, fax, USPS mail, or notarize it online - right from your account. Create an account now and try it yourself.
How do I execute as my physician online?
pdfFiller has made filling out and eSigning as my physician easy. The solution is equipped with a set of features that enable you to edit and rearrange PDF content, add fillable fields, and eSign the document. Start a free trial to explore all the capabilities of pdfFiller, the ultimate document editing solution.
Can I create an electronic signature for signing my as my physician in Gmail?
Upload, type, or draw a signature in Gmail with the help of pdfFiller’s add-on. pdfFiller enables you to eSign your as my physician and other documents right in your inbox. Register your account in order to save signed documents and your personal signatures.
What is as my physician?
As your physician refers to designating a healthcare provider as your primary doctor for medical treatment.
Who is required to file as my physician?
Any individual seeking medical care or treatment may choose to designate a physician as their primary doctor.
How to fill out as my physician?
You can fill out the designation by providing your physician's name, address, contact information, and agreement to designate them as your primary healthcare provider.
What is the purpose of as my physician?
The purpose of designating a physician as your primary doctor is to ensure continuity of care and establish a long-term relationship with a healthcare provider.
What information must be reported on as my physician?
You must report your physician's full name, address, phone number, and signature along with your acknowledgment of designating them as your primary healthcare provider.
Fill out your as my physician online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
As My Physician is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
