Get the free Patient bFormsb - Appearance Implants amp Laser Dentistry
Show details
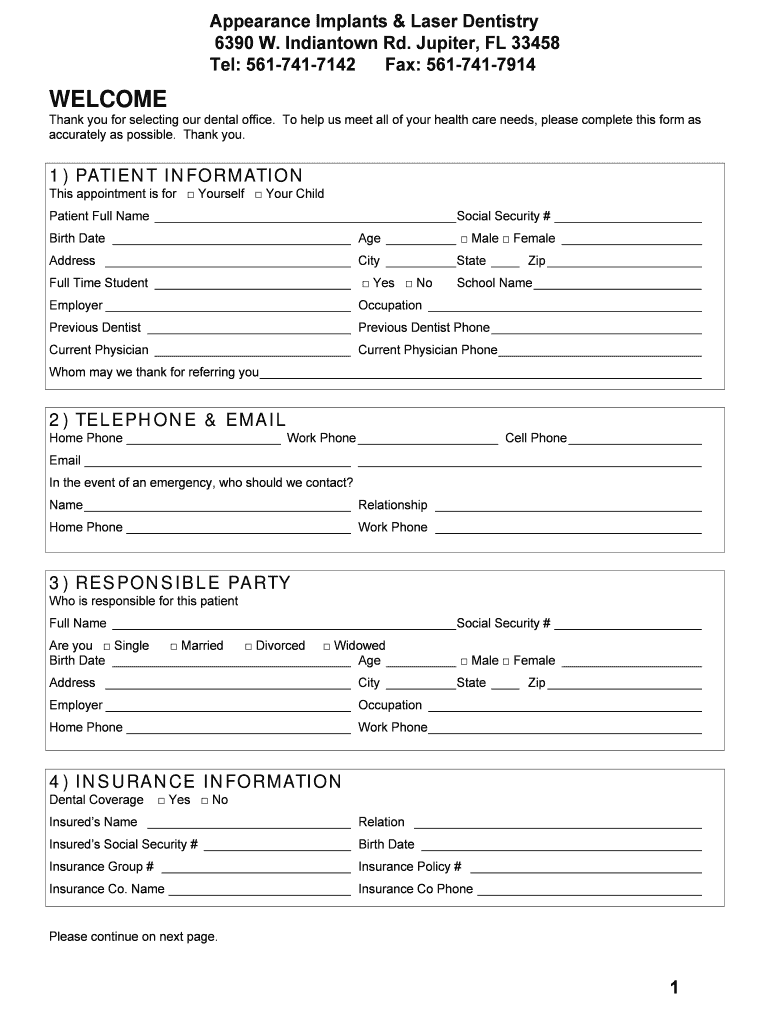
Appearance Implants & Laser Dentistry 6390 W. Indian town Rd. Jupiter, FL 33458 Tel: 5617417142 Fax: 5617417914 WELCOME Thank you for selecting our dental office. To help us meet all of your health
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign patient bformsb - appearance
Edit your patient bformsb - appearance form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your patient bformsb - appearance form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit patient bformsb - appearance online



To use the professional PDF editor, follow these steps:
1
Check your account. It's time to start your free trial.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit patient bformsb - appearance. Replace text, adding objects, rearranging pages, and more. Then select the Documents tab to combine, divide, lock or unlock the file.
4
Get your file. When you find your file in the docs list, click on its name and choose how you want to save it. To get the PDF, you can save it, send an email with it, or move it to the cloud.
It's easier to work with documents with pdfFiller than you can have ever thought. Sign up for a free account to view.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out patient bformsb - appearance
How to fill out patient forms - appearance:
01
Start by writing your full name in the designated space on the form. Make sure to write it clearly and legibly.
02
Next, provide your date of birth. Write the month, day, and year in the appropriate format as requested on the form.
03
Indicate your gender by checking the box or writing "M" for male or "F" for female.
04
If the form requires you to provide your address, write your complete residential address including street name, city, state, and zip code.
05
Some patient forms may ask for your contact information such as phone number and email address. Fill in these details accurately.
06
If there is a section for emergency contact information, provide the name, relationship, and contact details of someone who should be contacted in case of an emergency.
07
Some forms may ask for your marital status. Indicate whether you are single, married, divorced, widowed, or in another status as applicable.
08
If there is a space for occupation, write down your current or most recent occupation.
09
In the appearance section, you may be instructed to describe any distinguishing features or marks on your body. Provide accurate and relevant information.
10
Finally, review the completed form for any errors or missing information before submitting it.
Who needs patient forms - appearance?
01
Patients visiting healthcare facilities such as hospitals, clinics, or doctor's offices are typically required to fill out patient forms.
02
These forms are necessary for administrative purposes, gathering patient information, and maintaining accurate records.
03
Both new patients and returning patients may be asked to complete these forms in order to update their personal and medical information.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I modify patient bformsb - appearance without leaving Google Drive?
By combining pdfFiller with Google Docs, you can generate fillable forms directly in Google Drive. No need to leave Google Drive to make edits or sign documents, including patient bformsb - appearance. Use pdfFiller's features in Google Drive to handle documents on any internet-connected device.
How do I make changes in patient bformsb - appearance?
pdfFiller not only lets you change the content of your files, but you can also change the number and order of pages. Upload your patient bformsb - appearance to the editor and make any changes in a few clicks. The editor lets you black out, type, and erase text in PDFs. You can also add images, sticky notes, and text boxes, as well as many other things.
How can I fill out patient bformsb - appearance on an iOS device?
Download and install the pdfFiller iOS app. Then, launch the app and log in or create an account to have access to all of the editing tools of the solution. Upload your patient bformsb - appearance from your device or cloud storage to open it, or input the document URL. After filling out all of the essential areas in the document and eSigning it (if necessary), you may save it or share it with others.
What is patient forms - appearance?
The patient forms - appearance typically refers to the paperwork or documents that capture the physical characteristics of a patient such as height, weight, eye color, etc.
Who is required to file patient forms - appearance?
Medical professionals or healthcare providers are typically required to file patient forms - appearance for record-keeping and treatment purposes.
How to fill out patient forms - appearance?
Patient forms - appearance can usually be filled out by the patient themselves or with the assistance of a medical professional during a visit.
What is the purpose of patient forms - appearance?
The purpose of patient forms - appearance is to provide a baseline and reference point for healthcare providers to track any changes in the patient's physical characteristics over time.
What information must be reported on patient forms - appearance?
Information such as height, weight, hair color, eye color, skin tone, scars, and other physical traits may need to be reported on patient forms - appearance.
Fill out your patient bformsb - appearance online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Patient Bformsb - Appearance is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
