
Get the free Patient History Form Please Print - drjayparkcom
Show details
Patient History Form Please Print Today's Date: Name: Date of Birth: Primary Care Physician Referring Physician Please check yes or no for the following Past Medical History: Have you ever had any
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign patient history form please
Edit your patient history form please form online
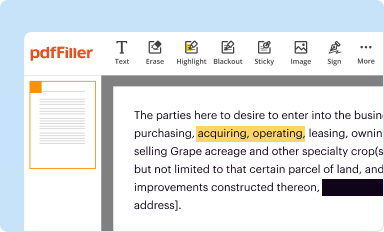
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
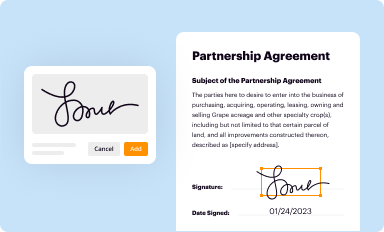
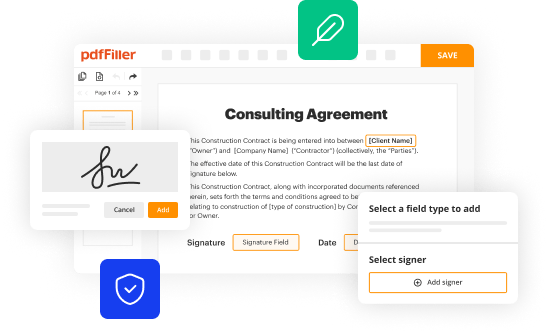
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
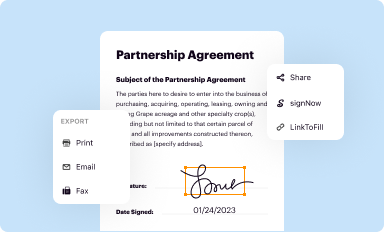
Share your form instantly
Email, fax, or share your patient history form please form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing patient history form please online



In order to make advantage of the professional PDF editor, follow these steps below:
1
Log in to account. Start Free Trial and sign up a profile if you don't have one yet.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit patient history form please. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
pdfFiller makes working with documents easier than you could ever imagine. Register for an account and see for yourself!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out patient history form please
How to fill out a patient history form:
01
Start by providing your personal information, such as your full name, date of birth, address, and contact details. This helps healthcare providers identify you correctly and reach out if needed.
02
Next, mention any relevant medical insurance details. This information is important for billing purposes and ensuring smooth processing of claims.
03
Provide a comprehensive medical history, including any pre-existing conditions, allergies, surgeries, or chronic illnesses. This helps doctors understand your overall health and make informed decisions regarding your treatment.
04
List all current medications you are taking, including prescription drugs, over-the-counter medications, and supplements. It is crucial to include the dosage and frequency of each medication to avoid potential drug interactions.
05
Mention any known family medical history, specifically any hereditary conditions or diseases that may have a genetic component. This information helps healthcare providers evaluate your risk factors accurately.
06
Provide details about your lifestyle habits, such as smoking, alcohol consumption, diet, and exercise routine. These factors can significantly impact your overall health and aid in devising an effective treatment plan.
07
If you have experienced any recent injuries or accidents, outline the details specifically. Include dates, circumstances, and any resultant treatments received.
08
Lastly, sign and date the form to certify that the information provided is accurate and complete to the best of your knowledge.
Who needs a patient history form:
01
Patients visiting a new healthcare provider or clinic may be required to fill out a patient history form. This helps the healthcare provider understand the patient's medical background and provide appropriate care.
02
Individuals who have experienced significant changes in their health, such as the development of new symptoms or the onset of a chronic condition, may need to update their patient history form. This ensures that healthcare providers have the most up-to-date information.
03
Patients undergoing a surgical procedure or seeking specialized treatment may also be required to fill out a patient history form to assess their suitability for the proposed treatment and minimize potential risks.
Remember, accurately filling out a patient history form is crucial for healthcare providers to make informed decisions and provide appropriate care.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I modify patient history form please without leaving Google Drive?
By integrating pdfFiller with Google Docs, you can streamline your document workflows and produce fillable forms that can be stored directly in Google Drive. Using the connection, you will be able to create, change, and eSign documents, including patient history form please, all without having to leave Google Drive. Add pdfFiller's features to Google Drive and you'll be able to handle your documents more effectively from any device with an internet connection.
How can I get patient history form please?
It's simple using pdfFiller, an online document management tool. Use our huge online form collection (over 25M fillable forms) to quickly discover the patient history form please. Open it immediately and start altering it with sophisticated capabilities.
How do I make changes in patient history form please?
With pdfFiller, the editing process is straightforward. Open your patient history form please in the editor, which is highly intuitive and easy to use. There, you’ll be able to blackout, redact, type, and erase text, add images, draw arrows and lines, place sticky notes and text boxes, and much more.
What is patient history form please?
The patient history form is a document that contains information about a patient's medical history, including past illnesses, surgeries, medications, allergies, and family medical history.
Who is required to file patient history form please?
Healthcare providers, such as doctors, nurses, and medical facilities, are typically required to have patients fill out a patient history form.
How to fill out patient history form please?
Patients can fill out the patient history form by providing accurate and detailed information about their medical history, including past illnesses, surgeries, medications, allergies, and family medical history.
What is the purpose of patient history form please?
The purpose of the patient history form is to provide healthcare providers with important information about a patient's medical background, which can help guide their treatment and care.
What information must be reported on patient history form please?
Patients must report information such as past illnesses, surgeries, medications, allergies, and family medical history on the patient history form.
Fill out your patient history form please online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Patient History Form Please is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
