
Get the free MEMBER/PHYSICIAN APPEAL/COMPLAINT FORM
Show details
MEMBER/PHYSICIAN APPEAL/COMPLAINT FORM Please print legibly below in black in. Form can be returned by mail, fax or email: Attention: Benefit Administration PO Box 2090 Buffalo, NY 142312090 Fax:
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign memberphysician appealcomplaint form
Edit your memberphysician appealcomplaint form form online
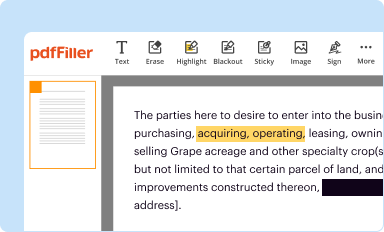
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
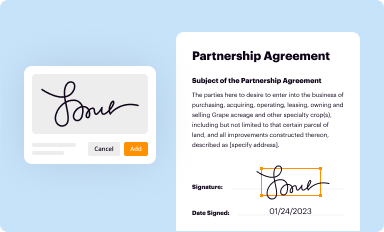
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
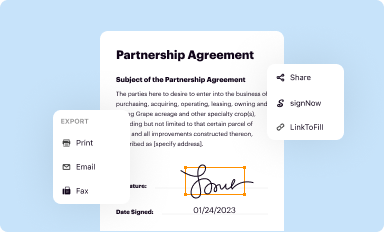
Share your form instantly
Email, fax, or share your memberphysician appealcomplaint form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit memberphysician appealcomplaint form online



To use our professional PDF editor, follow these steps:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Upload a file. Select Add New on your Dashboard and upload a file from your device or import it from the cloud, online, or internal mail. Then click Edit.
3
Edit memberphysician appealcomplaint form. Add and change text, add new objects, move pages, add watermarks and page numbers, and more. Then click Done when you're done editing and go to the Documents tab to merge or split the file. If you want to lock or unlock the file, click the lock or unlock button.
4
Save your file. Choose it from the list of records. Then, shift the pointer to the right toolbar and select one of the several exporting methods: save it in multiple formats, download it as a PDF, email it, or save it to the cloud.
With pdfFiller, dealing with documents is always straightforward.
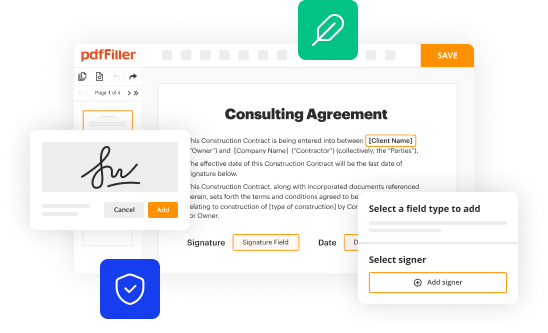
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out memberphysician appealcomplaint form
How to fill out memberphysician appealcomplaint form:
01
Start by filling out your personal information section, including your full name, contact details, and any relevant identification numbers. This will help the organization identify you and ensure that the appeal/complaint is being submitted by the correct person.
02
Move on to the details of the physician involved. Provide their name, contact information, and any other details that you have regarding their practice or affiliation. This will help the organization identify the physician in question and investigate the issue accordingly.
03
Clearly state the reason for your appeal or complaint. Provide a detailed explanation of the issue you are facing or the misconduct you believe has occurred. It is important to be specific and provide any supporting documentation or evidence to strengthen your case.
04
Be sure to include the date(s) and location(s) where the incident(s) took place, as well as any witnesses or other individuals involved. This will help the organization to conduct a thorough investigation and gain a better understanding of the situation.
05
If you have previously raised the issue with another department or individual within the organization, mention it in the form. Include any relevant details or responses you received, as this can provide additional context for your appeal or complaint.
06
Consider including any proposed resolutions or desired outcomes. Let the organization know what you hope to achieve by submitting the appeal or complaint. This can help guide their investigation and ensure that your concerns are addressed effectively.
Who needs memberphysician appealcomplaint form:
01
Patients who have experienced unsatisfactory treatment, misconduct, or other issues with their healthcare provider may need the memberphysician appealcomplaint form. This form allows them to formally raise their concerns and seek a resolution.
02
Individuals who believe that a physician has acted inappropriately, breached professional standards, or violated any codes of conduct may also need the memberphysician appealcomplaint form. This form provides a platform for them to report the misconduct and initiate an investigation.
03
Patients who have tried to resolve their issues through other means, such as direct communication with the medical facility or healthcare organization, and have not received a satisfactory response may find it necessary to utilize the memberphysician appealcomplaint form. This form serves as a formal escalation process to ensure that their concerns are taken seriously and properly addressed.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I complete memberphysician appealcomplaint form online?
Easy online memberphysician appealcomplaint form completion using pdfFiller. Also, it allows you to legally eSign your form and change original PDF material. Create a free account and manage documents online.
Can I create an eSignature for the memberphysician appealcomplaint form in Gmail?
Create your eSignature using pdfFiller and then eSign your memberphysician appealcomplaint form immediately from your email with pdfFiller's Gmail add-on. To keep your signatures and signed papers, you must create an account.
How do I fill out the memberphysician appealcomplaint form form on my smartphone?
Use the pdfFiller mobile app to complete and sign memberphysician appealcomplaint form on your mobile device. Visit our web page (https://edit-pdf-ios-android.pdffiller.com/) to learn more about our mobile applications, the capabilities you’ll have access to, and the steps to take to get up and running.
Fill out your memberphysician appealcomplaint form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Memberphysician Appealcomplaint Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
