
Get the free MEDICARE ENROLLMENT APPLICATION
Show details
This document is an application for Medicare enrollment intended for various suppliers, including clinics and group practices. It outlines the enrollment process, necessary supporting documentation,
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign medicare enrollment application
Edit your medicare enrollment application form online
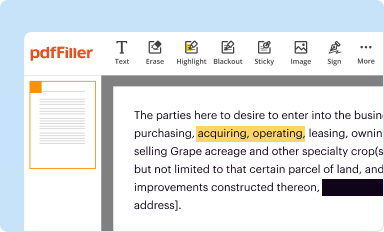
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
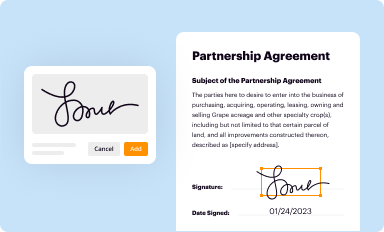
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
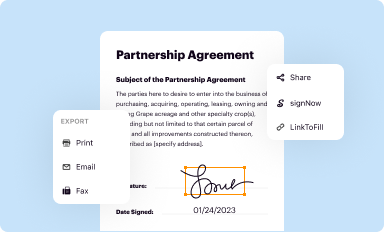
Share your form instantly
Email, fax, or share your medicare enrollment application form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing medicare enrollment application online



To use the services of a skilled PDF editor, follow these steps:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit medicare enrollment application. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Save your file. Select it in the list of your records. Then, move the cursor to the right toolbar and choose one of the available exporting methods: save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud.
With pdfFiller, it's always easy to work with documents.
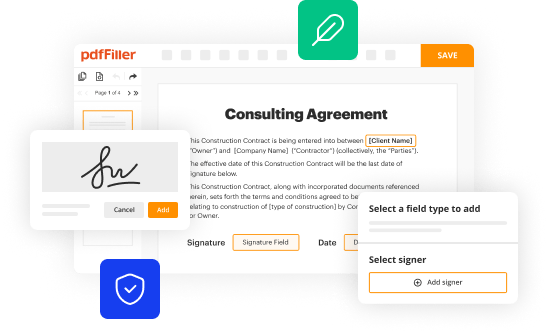
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out medicare enrollment application
How to fill out MEDICARE ENROLLMENT APPLICATION
01
Obtain the Medicare Enrollment Application form from the Social Security Administration (SSA) website or local office.
02
Read the instructions carefully to understand the requirements and information needed.
03
Fill out personal information, including your name, address, date of birth, and Social Security number.
04
Select the type of Medicare coverage you wish to enroll in (Part A, Part B, or both).
05
Indicate any additional coverage you have, such as employer insurance.
06
Provide information about your current or previous health coverage, if applicable.
07
Review your application for accuracy and completeness.
08
Sign and date the application at the designated section.
09
Submit the completed application to your local SSA office or online if applicable.
Who needs MEDICARE ENROLLMENT APPLICATION?
01
Individuals who are 65 years or older.
02
People under 65 with specific disabilities.
03
Individuals with End-Stage Renal Disease (ESRD) or Amyotrophic Lateral Sclerosis (ALS).
04
Those who want to protect their healthcare needs as they age or if they have qualifying conditions.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is MEDICARE ENROLLMENT APPLICATION?
The Medicare Enrollment Application is a form that individuals must complete to enroll in the Medicare program, which provides health insurance for people aged 65 and older, as well as certain younger individuals with disabilities.
Who is required to file MEDICARE ENROLLMENT APPLICATION?
Individuals who are eligible for Medicare, typically those aged 65 and older, as well as younger individuals with qualifying disabilities or specific conditions, are required to file the Medicare Enrollment Application.
How to fill out MEDICARE ENROLLMENT APPLICATION?
To fill out the Medicare Enrollment Application, individuals must provide personal information such as their name, address, date of birth, social security number, and details about their current health insurance. The application can be completed online or by submitting a paper form.
What is the purpose of MEDICARE ENROLLMENT APPLICATION?
The purpose of the Medicare Enrollment Application is to facilitate the enrollment process into Medicare, allowing eligible individuals to access healthcare services covered under the Medicare program.
What information must be reported on MEDICARE ENROLLMENT APPLICATION?
The information that must be reported on the Medicare Enrollment Application includes personal details such as full name, address, date of birth, Social Security number, employment history, and any existing health insurance coverage.
Fill out your medicare enrollment application online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Medicare Enrollment Application is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
