Last updated on May 2, 2026

Get the free Health Care/Dependent Care Claim Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
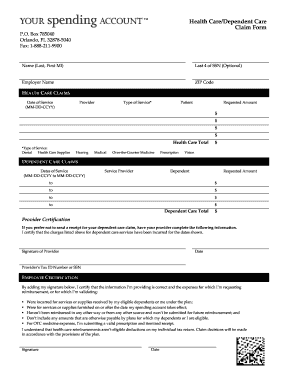
What is Care Claim Form
The Health Care/Dependent Care Claim Form is a personal finance document used by employees to request reimbursement for qualifying health and dependent care expenses.
pdfFiller scores top ratings on review platforms
Who needs Care Claim Form?
Explore how professionals across industries use pdfFiller.

Care Claim Form is needed by:
-
Employees seeking reimbursement for health care expenses
-
Employees submitting claims for dependent care costs
-
Providers needing to verify services for reimbursements
-
Human Resources personnel managing employee benefits
-
Financial advisors assisting clients with spending accounts
Comprehensive Guide to Care Claim Form
What is the Health Care/Dependent Care Claim Form?
The Health Care/Dependent Care Claim Form is essential for employees in Florida seeking reimbursement for eligible health care and dependent care expenses. This form serves as a crucial tool for managing personal finances effectively.
This form not only provides a structured way to request reimbursements but also emphasizes the importance of utilizing health care and dependent care services. Employees are encouraged to understand its significance in ensuring they are compensated for necessary expenses.
Purpose and Benefits of the Health Care/Dependent Care Claim Form
The primary advantage of completing the Health Care/Dependent Care Claim Form is the facilitation of timely reimbursements for eligible expenses. By using this form, employees can manage their health care and dependent care expenditures more efficiently.
Maintaining financial health is crucial, and completing this form helps employees maximize their spending accounts. This capability is vital for managing budgets and ensuring expenses are accounted for accurately.
Key Features of the Health Care/Dependent Care Claim Form
Within the Health Care/Dependent Care Claim Form, there are several critical elements that users should be aware of. The form includes various fillable fields such as provider details, expense amounts, and signatures that are crucial for validation.
-
Fillable fields for essential information, such as Name and Social Security Number
-
Sections detailing amounts and provider specifics
-
Importance of attaching original receipts for expenses
Who Needs the Health Care/Dependent Care Claim Form?
The audience for this claim form primarily includes employees who incur qualified expenditures for health care and dependent care related to their dependents. Understanding the eligibility criteria is vital for those wishing to utilize the form for reimbursements.
Employees should be aware of what constitutes a qualified expense, ensuring that they are correctly filling out the dependent care reimbursement form based on specific guidelines for Florida residents.
How to Fill Out the Health Care/Dependent Care Claim Form Online (Step-by-Step)
Filling out the Health Care/Dependent Care Claim Form online can be streamlined through pdfFiller’s platform. Here’s a step-by-step guide on how to complete the form digitally:
-
Access the form on pdfFiller’s platform.
-
Fill in your personal information, including Name and Social Security Number.
-
Enter required expense details, including amounts and provider information.
-
Attach scanned copies of original receipts.
-
Sign the form digitally.
-
Submit the completed form via preferred methods (fax or mail).
Submission Methods and Delivery of the Health Care/Dependent Care Claim Form
Once the Health Care/Dependent Care Claim Form is completed, users have several submission options available. These methods include faxing or mailing the completed document to your designated spending account.
-
Submitting via fax for immediate processing
-
Mailing the form, ensuring to send it to the correct address
It is recommended to follow best practices when submitting the form to ensure timely handling and processing of claims.
Confirmation and Tracking After Submission
After submitting the Health Care/Dependent Care Claim Form, users can expect confirmation of receipt. It is essential to know how to confirm that your claim form has been received and to track its status effectively.
-
Contact the processing department for confirmation
-
Utilize available tools provided by your company for tracking submission status
Common Errors and How to Avoid Them When Completing the Claim Form
While filling out the Health Care/Dependent Care Claim Form, users may encounter common errors that could impede successful submission. Identifying these mistakes in advance can save time and frustration.
-
Incorrectly filling out mandatory fields
-
Failing to attach original receipts
-
Missing signatures from necessary parties
Tips for avoiding these issues include double-checking all entries and ensuring all required documents are included.
Security and Compliance for Your Health Care/Dependent Care Claim Form
When using pdfFiller to complete and submit your Health Care/Dependent Care Claim Form, it’s crucial to be assured about the security of your information. The platform employs 256-bit encryption and complies with HIPAA regulations to protect sensitive data.
Using a trusted platform like pdfFiller is essential when handling personal documents, ensuring that your health care reimbursement form is secure throughout the process.
Simplifying the Process with pdfFiller
pdfFiller offers substantial features that simplify the process of filling out the Health Care/Dependent Care Claim Form. The platform's capabilities enhance user experience by making form management efficient.
-
Seamless document editing and signing
-
User-friendly interface that streamlines form filling and submission
Testimonials from satisfied users further highlight the effectiveness of pdfFiller in managing such important forms.
How to fill out the Care Claim Form
-
1.Access pdfFiller and search for the Health Care/Dependent Care Claim Form in the document library.
-
2.Open the form and familiarize yourself with the available fillable fields including name, social security number, and address.
-
3.Before starting, gather all necessary information such as dates of service, providers, and amounts paid.
-
4.Use the interface to click on each fillable field and enter the requested information accordingly.
-
5.Make sure to use the checkboxes and tables provided to accurately describe your services and expenses.
-
6.Attach original receipts by scanning or uploading them through pdfFiller, as they are required for submission.
-
7.Review the completed form thoroughly to ensure that all fields are filled out correctly and both the employee and provider signatures are included.
-
8.Finalize the form by using pdfFiller’s options to save and download a copy for your records.
-
9.To submit the form, choose the fax or mail option and follow the directions for sending it to Your Spending Account for processing.

What are the eligibility requirements for using this form?
Employees must have incurred eligible health care or dependent care expenses and be enrolled in a spending account to use the Health Care/Dependent Care Claim Form.
Are there deadlines for submitting the claim form?
Yes, claims should be submitted within the specified deadlines set by the spending account provider to ensure reimbursement. Refer to your spending account policy for specific timeframes.
What methods can I use to submit this form?
The completed Health Care/Dependent Care Claim Form can be submitted via fax or through mail directly to Your Spending Account. Ensure to verify the correct submission address.
What supporting documents are required with the form?
You must attach original receipts that detail the services provided and related expenses along with the completed claim form to support your reimbursement request.
What common mistakes should I avoid when completing the form?
Common mistakes include failing to sign the document, not providing complete information, or forgetting to attach original receipts. Double-check all entries before submission.
How long does processing typically take?
Processing times can vary, but most claims are usually processed within a few weeks. Check with Your Spending Account for more detailed information on processing times.
What should I do if I encounter problems with the form?
If you face any issues while filling out the form, consult the help section on pdfFiller or contact Your Spending Account's customer service for assistance.
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.