
Get the free formulario de pacientes
Show details
FORMULARIO DE REGISTRO DE PACIENTES NUEVOS 900 Avenida Acaso Suite A Camarillo CA 93012 LLAMADA SIN COSTO 800-376-4968 TEL FONO 805-388-9336 FAX 805-482-6324 INFORMACI N DEL PACIENTE Adjunte una copia de la licencia de conducir frente y rev s PRIMER NOMBRE APELLIDO INICIALES SEGUNDO NOMBRE FECHA DE NACIMIENTO N. SS TEL FONO CELULAR EDAD MASCULINO FEMENINO DIRECCI N DE CORREO ELECTR NICO LA RESIDENCIA TRABAJO CIUDAD/ESTADO Y C DIGO POSTAL DE CASA DE OFICINA FAX Si es distinta a la anterior...
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign formulario de pacientes
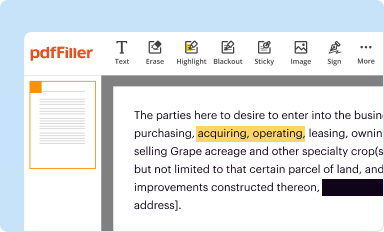
Edit your formulario de pacientes form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
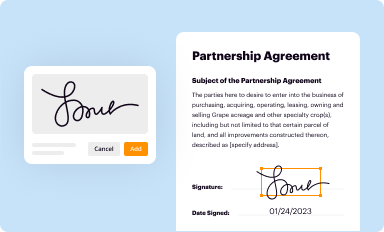
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
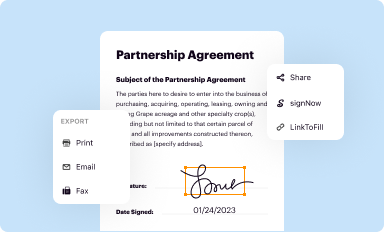
Share your form instantly
Email, fax, or share your formulario de pacientes form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing formulario de pacientes online



To use our professional PDF editor, follow these steps:
1
Log in to your account. Click Start Free Trial and sign up a profile if you don't have one.
2
Upload a file. Select Add New on your Dashboard and upload a file from your device or import it from the cloud, online, or internal mail. Then click Edit.
3
Edit formulario de pacientes. Rearrange and rotate pages, insert new and alter existing texts, add new objects, and take advantage of other helpful tools. Click Done to apply changes and return to your Dashboard. Go to the Documents tab to access merging, splitting, locking, or unlocking functions.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
pdfFiller makes working with documents easier than you could ever imagine. Register for an account and see for yourself!
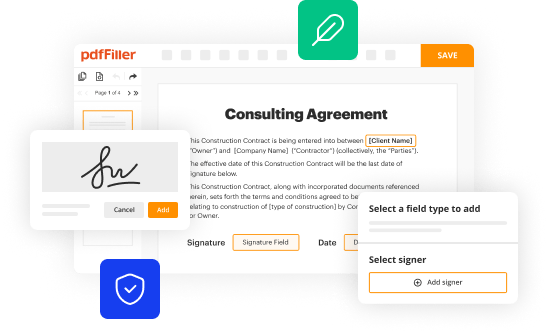
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out formulario de pacientes
How to fill out formulario de registro de:
01
Start by carefully reading the instructions on the form. Make sure you understand all the fields and requirements.
02
Begin by providing your personal information such as your full name, date of birth, address, and contact details. This is necessary for identification purposes.
03
Proceed to fill out any additional information required, such as your occupation, marital status, and nationality. These details may vary depending on the specific form.
04
Pay attention to any specific sections that require supporting documentation. For example, you may need to attach copies of your ID card, passport, or other relevant documents.
05
If the form includes questions or sections related to your health or any legal matters, answer them accurately and truthfully. Provide any necessary medical or legal documentation if required.
06
Double-check all the information you have provided before submitting the form. Ensure that all the fields are complete and accurate. This will help avoid any delays or complications in processing your registration.
Who needs formulario de registro de:
01
Individuals who are applying for a specific service, program, or membership that requires registration may need to fill out formulario de registro de. This could include registering for a course, applying for a job, or joining a club or organization.
02
Companies or organizations may also require participants or customers to fill out formulario de registro de as part of their registration process. This helps them gather necessary information and maintain a record of their clientele.
03
Government institutions may use formulario de registro de for various purposes, such as registering for census data, applying for permits or licenses, or enrolling in public welfare programs.
Fill
form
: Try Risk Free
People Also Ask about
¿Qué es un registro de datos de pacientes?
Un registro de pacientes recopila información sobre un grupo de pacientes que padecen una enfermedad en particular. Los registros son bases de datos que contienen datos cuantitativos y cualitativos sobre los pacientes. Los registros juegan un papel crucial en el desarrollo de terapias para las enfermedades raras.
¿Cómo llenar un formulario médico?
Consejos para aplicar un formulario médico Incluye el nombre y la información de contacto del médico del paciente. Agrega una sección que incluya los comentarios de seguimiento del médico. Incluye una sección de “progreso” en la que se anoten todas las actualizaciones y cambios.
¿Cómo se hace un registro de pacientes?
Datos básicos. Anota el nombre del paciente, edad, altura, peso y principal dolencia o dolencias. Reúne la historia primaria. Amplia con la historia secundaria. Toma la historia terciaria. Incluye la revisión de los síntomas. Entrevista al paciente para hacer un historial médico pasado.
¿Qué es y qué contiene un registro clínico?
Con el registro clínico electrónico es posible adjuntar documentos, imágenes y vídeos de los procedimientos, garantizando que todas las informaciones médicas del paciente estarán reunidas en un mismo archivo (el Registro Electrónico de Salud) y facilitando el acceso del médico a todos esos datos relevantes.
¿Qué debe llevar un registro clínico?
¿Cómo se debe hacer el registro clínico? Este debe ser de manera clara, legible, sin tachones, enmendaduras, intercalaciones y sin dejar espacios en blanco. Cada anotación debe llevar la fecha y hora en la que se realiza, con el nombre completo y firma del autor de la misma.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I send formulario de pacientes to be eSigned by others?
formulario de pacientes is ready when you're ready to send it out. With pdfFiller, you can send it out securely and get signatures in just a few clicks. PDFs can be sent to you by email, text message, fax, USPS mail, or notarized on your account. You can do this right from your account. Become a member right now and try it out for yourself!
How can I edit formulario de pacientes on a smartphone?
You can easily do so with pdfFiller's apps for iOS and Android devices, which can be found at the Apple Store and the Google Play Store, respectively. You can use them to fill out PDFs. We have a website where you can get the app, but you can also get it there. When you install the app, log in, and start editing formulario de pacientes, you can start right away.
How can I fill out formulario de pacientes on an iOS device?
pdfFiller has an iOS app that lets you fill out documents on your phone. A subscription to the service means you can make an account or log in to one you already have. As soon as the registration process is done, upload your formulario de pacientes. You can now use pdfFiller's more advanced features, like adding fillable fields and eSigning documents, as well as accessing them from any device, no matter where you are in the world.
What is formulario de pacientes?
Formulario de pacientes is a patient form used in healthcare settings to collect essential information about a patient's medical history, current health status, and personal details.
Who is required to file formulario de pacientes?
Patients visiting a healthcare facility or seeking medical treatment are required to fill out the formulario de pacientes.
How to fill out formulario de pacientes?
To fill out formulario de pacientes, provide accurate personal details, medical history, current medications, allergies, and any relevant health information requested on the form.
What is the purpose of formulario de pacientes?
The purpose of formulario de pacientes is to ensure healthcare providers have comprehensive information about the patient to deliver appropriate care and treatment.
What information must be reported on formulario de pacientes?
The information that must be reported on formulario de pacientes includes the patient's name, contact information, medical history, current medications, allergies, and insurance details if applicable.
Fill out your formulario de pacientes online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Formulario De Pacientes is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
