Last updated on Apr 10, 2026

Get the free Direct Member Reimbursement Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is direct member reimbursement form
The Direct Member Reimbursement Form is a medical billing document used by employees or patients to request reimbursement for prescription costs.
pdfFiller scores top ratings on review platforms
Who needs direct member reimbursement form?
Explore how professionals across industries use pdfFiller.

Direct member reimbursement form is needed by:
-
Employees who incur prescription medication costs
-
Patients seeking reimbursement for healthcare expenses
-
Human resources personnel managing employee benefits
-
Pharmacies submitting claims for reimbursements
-
Insurance companies processing claims
-
Healthcare administrators overseeing billing
Comprehensive Guide to direct member reimbursement form
What is the Direct Member Reimbursement Form?
The Direct Member Reimbursement Form is a vital document in the healthcare reimbursement process, enabling employees and patients to request reimbursement for prescription costs. This form plays a key role in simplifying the reimbursement experience by allowing users to provide necessary information regarding their expenses. To submit this form, individuals must meet specific requirements, including providing supporting documentation.
Purpose and Benefits of the Direct Member Reimbursement Form
Utilizing the Direct Member Reimbursement Form significantly streamlines the reimbursement process for employees and patients. The benefits of using this form include:
-
Faster processing of reimbursement requests
-
Clearer record-keeping of prescription expenditures
-
Enhanced convenience for managing healthcare expenses
It is crucial for users to include detailed prescription information to ensure a smooth submission process.
Who Needs the Direct Member Reimbursement Form?
This form is primarily intended for employees and patients in New York who have incurred prescription expenses. Eligibility for using the Direct Member Reimbursement Form is determined by scenarios such as:
-
Employees purchasing medications as part of employment benefits
-
Patients seeking reimbursement for out-of-pocket prescription costs
Only eligible individuals can fill out and sign the form to initiate the reimbursement process.
How to Fill Out the Direct Member Reimbursement Form Online (Step-by-Step)
Filling out the Direct Member Reimbursement Form online can be efficiently done by following these steps:
-
Access the online form through the appropriate platform.
-
Enter your employee or patient data, including your name and identification details.
-
Provide all relevant prescription information, including medication names and costs.
-
Complete any required fields, ensuring proper signatures are included.
-
Review the form for accuracy before submission.
Tips for success include double-checking all entries for accuracy and ensuring that required fields are not left blank.
Field-by-Field Instructions
When completing the Direct Member Reimbursement Form, specific information must be accurately provided in each field. Key fields include:
-
Employee’s Name
-
Patient’s Name
-
Date of Purchase
Common mistakes to avoid involve leaving fields incomplete or misrepresenting prescription details. Providing accurate information is essential along with any necessary supporting receipts.
Required Documents and Supporting Materials
To ensure successful submission of the Direct Member Reimbursement Form, individuals need to gather essential documentation, including:
-
Original or digital pharmacy receipts
-
Identification proofs
-
Any additional documents requested by the processing authority
Keeping copies of all submitted documents is important for personal record-keeping, especially when submitting digitally.
Submission Methods and Processing Time
There are multiple methods available for submitting the completed Direct Member Reimbursement Form:
-
Mailing the form to ProAct Pharmacy Services
-
Faxing the completed document
-
Submitting the form online
After submission, processing times may vary. Users should expect some delays depending on submission method and volume, and they can track the status of their reimbursement request once it has been submitted.
Security and Compliance for the Direct Member Reimbursement Form
You can have confidence in the security of your personal information when using the Direct Member Reimbursement Form. pdfFiller implements stringent security measures, including encryption and compliance with HIPAA regulations, to protect sensitive health documents. To maintain privacy during the submission process, consider best practices such as using secure connections and ensuring that documents are submitted through trusted platforms.
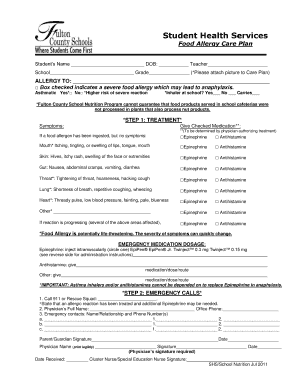
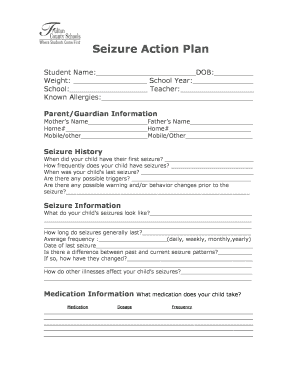
Sample or Example of a Completed Direct Member Reimbursement Form
To assist users in properly completing the Direct Member Reimbursement Form, a filled-out sample form is available for reference. This visual aid helps clarify common areas, with annotations highlighting important fields and instructions on interpreting the information accurately.
Utilize pdfFiller for Your Direct Member Reimbursement Form
For a seamless experience when filling out the Direct Member Reimbursement Form, consider using pdfFiller. The platform allows you to edit, sign, and submit documents easily while managing your healthcare files securely. Features such as easy editing and enhanced support for handling sensitive information make pdfFiller an excellent choice for your form-filling needs.
How to fill out the direct member reimbursement form
-
1.Access the Direct Member Reimbursement Form by visiting pdfFiller and searching for the form name in the search bar.
-
2.Open the form by clicking on it in the search results to launch the online editor.
-
3.Before you begin filling out the form, gather necessary documents such as pharmacy receipts, and relevant insurance information about the prescription.
-
4.Locate the blank fields on the form including 'Employee’s Name:', 'Patient’s Name:', and 'Date'. Click on each field to enter the required information.
-
5.To add your signature, click on the 'Signature' field. Use the drawing tool or upload a scanned signature for completion.
-
6.Review all the inputted information for accuracy and completeness, ensuring all required sections are filled out correctly.
-
7.Once everything is validated, click on the save option to keep a copy of your completed form.
-
8.You can download the form to your device or submit it directly through the platform to ProAct Pharmacy Services for processing.

Who is eligible to use the Direct Member Reimbursement Form?
The Direct Member Reimbursement Form is designed for employees and patients who have incurred expenses for prescription medications and are seeking reimbursement from their employer or insurance provider.
What documents do I need to submit with this reimbursement form?
You will need to submit pharmacy receipts, proof of payment, and any relevant insurance documentation along with the completed form for processing.
How do I submit the filled-out Direct Member Reimbursement Form?
The completed form can be submitted directly through pdfFiller or downloaded and sent via email or regular mail to ProAct Pharmacy Services, as specified in the form instructions.
Are there any common mistakes to avoid when filling out the form?
Common mistakes include missing required fields, submitting without a signature, or forgetting to include supporting documents like receipts. Double-check all entries before submission.
What are typical processing times for reimbursement requests?
Processing times can vary, but generally, you can expect to receive reimbursement within 2-4 weeks after your form has been submitted and accepted by the processing entity.
Can I modify the form after I've started filling it out?
Yes, pdfFiller allows you to modify the form at any point until you save and finalize your entry. Make sure to review any changes made before submission.
What is the purpose of the Direct Member Reimbursement Form?
The purpose of the Direct Member Reimbursement Form is to provide a structured way for employees or patients to request reimbursement for eligible prescription costs incurred.
Related Content
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.