MI WC-100 2011 free printable template
Show details
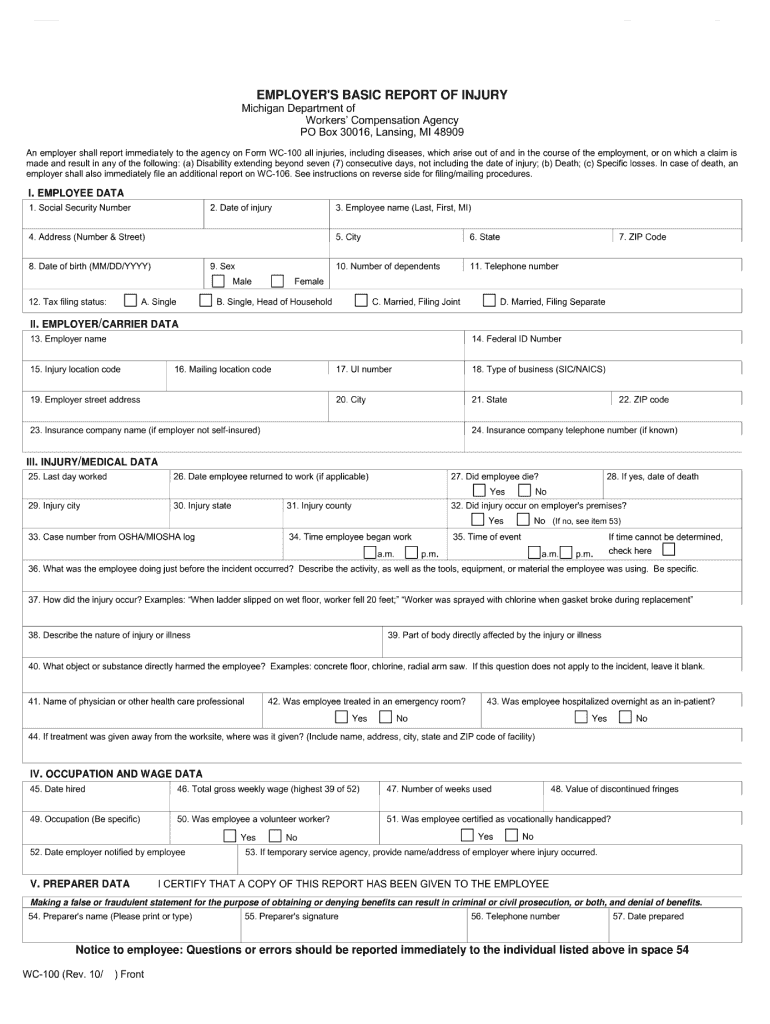
Go to Instructions Print Reset EMPLOYER S BASIC REPORT OF INJURY Michigan Department of Workers Compensation Agency PO Box 30016 Lansing MI 48909 An employer shall report immedia tely to the agen cy on Form WC-100 all injuries including diseases which arise out of and in the course of the employment or on which a claim is made and result in any of the following a Disability extending beyond seven 7 consecutive days not including the date of injury b Death c Specific losses. 54. Preparer s...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign MI WC-100

Edit your MI WC-100 form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your MI WC-100 form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit MI WC-100 online



To use the services of a skilled PDF editor, follow these steps below:
1
Log in to your account. Start Free Trial and sign up a profile if you don't have one.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit MI WC-100. Rearrange and rotate pages, insert new and alter existing texts, add new objects, and take advantage of other helpful tools. Click Done to apply changes and return to your Dashboard. Go to the Documents tab to access merging, splitting, locking, or unlocking functions.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
With pdfFiller, dealing with documents is always straightforward. Try it now!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
MI WC-100 Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out MI WC-100

How to fill out MI WC-100
01
Begin by downloading the MI WC-100 form from the Michigan Department of Labor and Economic Opportunity website.
02
Fill in your personal information, including your name, address, and social security number in the designated sections.
03
Provide details about your employer, including the company name, address, and contact information.
04
Describe the nature of your injury or illness, including when and where it occurred.
05
Specify the date you first noticed symptoms or were injured.
06
List all medical providers you have seen for treatment related to this injury or illness.
07
Sign and date the form to certify that the information provided is accurate.
08
Submit the completed form to your employer and retain a copy for your records.
Who needs MI WC-100?
01
Employees who have sustained a work-related injury or illness in Michigan.
02
Workers seeking workers' compensation benefits for their medical treatment and lost wages.
03
Employers who need to file a claim for their injured employees.
Instructions and Help about MI WC-100
Fill
form
: Try Risk Free
People Also Ask about
What is the EMPLOYERS first report of injury in PA?
Form LIBC-344 First Report of Injury (FROI). As soon as you have been notified of a work-related injury, please fill out this form and submit it to EMPLOYERS. This form must be completed within 10 days from notice of a work-related injury. Fatalities must be reported within 24 hours.
What form is employee first report of injury in Texas?
Form DWC-1 Employer's First Report of Injury or Occupational Disease. The employer is required to submit this form with EMPLOYERS and the injured employee or the injured employee's attorney within eight days after the employee's absence from work or notice of the Injury or Occupational Disease.
What is the EMPLOYERS responsibility when a worker is injured?
Employer Responsibilities If an employee is injured, you are responsible for making sure that a First Report of Injury, or other similar document, is completed and forwarded to your workers' compensation carrier. You are responsible for making sure that you do not violate any laws or rights of the injured employee.
What is a DWC 7 form?
DWC-7 Notice to Employees-Injuries Caused by Work (English and Spanish). This form provides your employees with information regarding workers' compensation benefits and the Medical Provider Network (MPN) in California.
What is the IL form 45?
IC45 First Report of Injury (FROI). Section 6(b) of the Workers' Compensation Act requires that you (or insurers acting on your behalf) send reports to the Illinois Workers' Compensation Commission on all accidents involving more than three lost work days.
What is a DWC005 form?
DWC005, Employer Notice of No Coverage or Termination of Coverage. DWC020SI, Self-Insured Governmental Entity Coverage Information. Steps to electronically submit a form to the Division of Workers' Compensation: Open the form: Google Chrome and Microsoft Edge.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I edit MI WC-100 on a smartphone?
The pdfFiller apps for iOS and Android smartphones are available in the Apple Store and Google Play Store. You may also get the program at https://edit-pdf-ios-android.pdffiller.com/. Open the web app, sign in, and start editing MI WC-100.
How do I complete MI WC-100 on an iOS device?
Download and install the pdfFiller iOS app. Then, launch the app and log in or create an account to have access to all of the editing tools of the solution. Upload your MI WC-100 from your device or cloud storage to open it, or input the document URL. After filling out all of the essential areas in the document and eSigning it (if necessary), you may save it or share it with others.
Can I edit MI WC-100 on an Android device?
With the pdfFiller mobile app for Android, you may make modifications to PDF files such as MI WC-100. Documents may be edited, signed, and sent directly from your mobile device. Install the app and you'll be able to manage your documents from anywhere.
What is MI WC-100?
MI WC-100 is a form used in Michigan for reporting workers' compensation claims and related information to the Michigan Workers' Compensation Agency.
Who is required to file MI WC-100?
Employers who have employees that sustain work-related injuries and wish to report these claims for workers' compensation benefits are required to file MI WC-100.
How to fill out MI WC-100?
To fill out MI WC-100, employers must provide details about the employee's injury, circumstances of the incident, employer information, and any other required data specified on the form.
What is the purpose of MI WC-100?
The purpose of MI WC-100 is to ensure that the Michigan Workers' Compensation Agency receives accurate information about workplace injuries for the proper processing of claims and benefits.
What information must be reported on MI WC-100?
Information that must be reported on MI WC-100 includes the employee's name and address, date of injury, nature of injury, wage information, and details of any medical treatment received.
Fill out your MI WC-100 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
MI WC-100 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
