
Get the free Health Benefit Claim Form
Show details
This form is used by insured students at Boise State University to file health benefit claims for injuries or sicknesses, detailing the necessary information regarding the patient and the circumstances
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign health benefit claim form
Edit your health benefit claim form form online
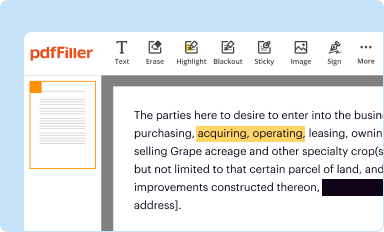
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
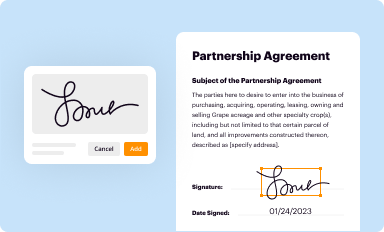
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
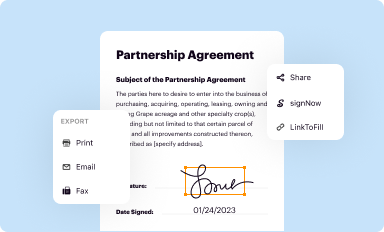
Share your form instantly
Email, fax, or share your health benefit claim form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing health benefit claim form online



To use the services of a skilled PDF editor, follow these steps:
1
Log in to your account. Start Free Trial and sign up a profile if you don't have one yet.
2
Upload a file. Select Add New on your Dashboard and upload a file from your device or import it from the cloud, online, or internal mail. Then click Edit.
3
Edit health benefit claim form. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
With pdfFiller, it's always easy to work with documents.
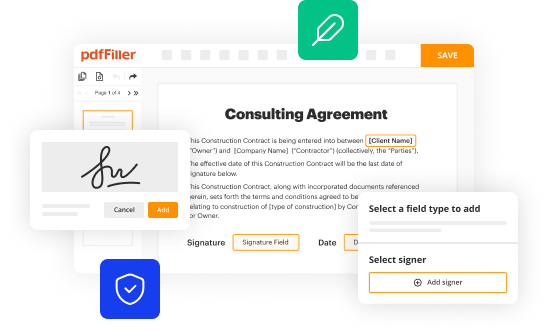
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out health benefit claim form
How to fill out Health Benefit Claim Form
01
Obtain a copy of the Health Benefit Claim Form from your insurance provider.
02
Fill in your personal information, including your name, address, and policy number.
03
Provide the details of the healthcare service received, including the date, provider's name, and service description.
04
List any applicable charges and attach relevant receipts or invoices for the services.
05
Sign and date the form to certify that the information provided is accurate.
06
Submit the completed claim form along with any supporting documents to your insurance company, either by mail or electronically, as instructed.
Who needs Health Benefit Claim Form?
01
Individuals with health insurance seeking reimbursement for medical expenses.
02
Patients who have received healthcare services covered by their insurance plan.
03
Subscribers of group health plans through employers or organizations.
Fill
form
: Try Risk Free
People Also Ask about
What does the HCFA form stand for?
If you wonder what HCFA stands for, it's the "Health Care Financing Administration," a federal agency responsible for administering the Medicare and Medicaid programs in the United States.
What was the HCFA previously known as?
"HCFA" stands for the Health Care Financing Administration, which was the previous name of the Centers for Medicare & Medicaid Services (CMS), the federal agency responsible for administering Medicare, Medicaid, and other healthcare programs.
How do I fill out a reimbursement claim form?
Follow the steps given below to file a reimbursement health insurance claim: Step 1: Inform the Insurance Company. Step 2: Obtain Treatment. Step 3: Pay the Hospital Bill. Step 4: Collect All Your Documents. Step 5: Fill up the Claim Form. Step 6: Submit All Documents to the Insurance Company.
What is a claim form for insurance?
TTK Revised Claim Form 1 © Wikimedia Commons Claim Form legal definition: A claim form is defined as a formal written request to an insurance company, the government, or other entity for compensation you believe you are entitled to under their rules or statutes.
What is a HCFA form?
However, the term HCFA is still commonly used to refer to the standard claim form used by healthcare providers to bill Medicare and some private insurance companies. The form is officially known as the HCFA-1500, but it is also sometimes called the CMS-1500 or simply the "medical claim form."
What is the difference between CMS 1500 and HCFA 1500?
The term CMS 1500 refers to the Centers for Medicare & Medicaid Services Form 1500, while HCFA 1500 is an older term that stands for Health Care Financing Administration Form 1500. The HCFA was renamed CMS in the year 2001, but the term HCFA 1500 is still widely accepted and used in the industry.
What is a hicf?
However, changes within the last five years or so have mandated that health care providers complete what is known as a Health Insurance Claim Form (HICF or HICA) along with the other required paperwork.
How to write a cover letter for a health insurance claim?
How to Draft a Health Insurance Claim Letter Identify Your Basic Information. Compose a Formal Greeting. Express the Purpose of Your Letter. Brief Description of Medical Treatment. Provide Details of the Costs Involvement. Attach Required Documents. Prompt Processing Request. Closing Statement.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is Health Benefit Claim Form?
The Health Benefit Claim Form is a document used by individuals to request reimbursement for medical expenses covered under their health insurance plan.
Who is required to file Health Benefit Claim Form?
Typically, the insured individual or the healthcare provider on behalf of the individual is required to file the Health Benefit Claim Form to receive reimbursement for healthcare services rendered.
How to fill out Health Benefit Claim Form?
To fill out the Health Benefit Claim Form, individuals must provide personal information, details of the medical services received, itemized bills, dates of service, and any required signatures or authorizations.
What is the purpose of Health Benefit Claim Form?
The purpose of the Health Benefit Claim Form is to facilitate the process of requesting reimbursement from an insurance company for eligible medical expenses incurred by the policyholder.
What information must be reported on Health Benefit Claim Form?
The information that must be reported includes the claimant's identification details, insurance policy number, provider information, description of services rendered, dates of service, and total charges incurred.
Fill out your health benefit claim form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Health Benefit Claim Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
