Get the free Primary Care bProvider Applicationb Form - Arizona Department of bb - azdhs
Show details
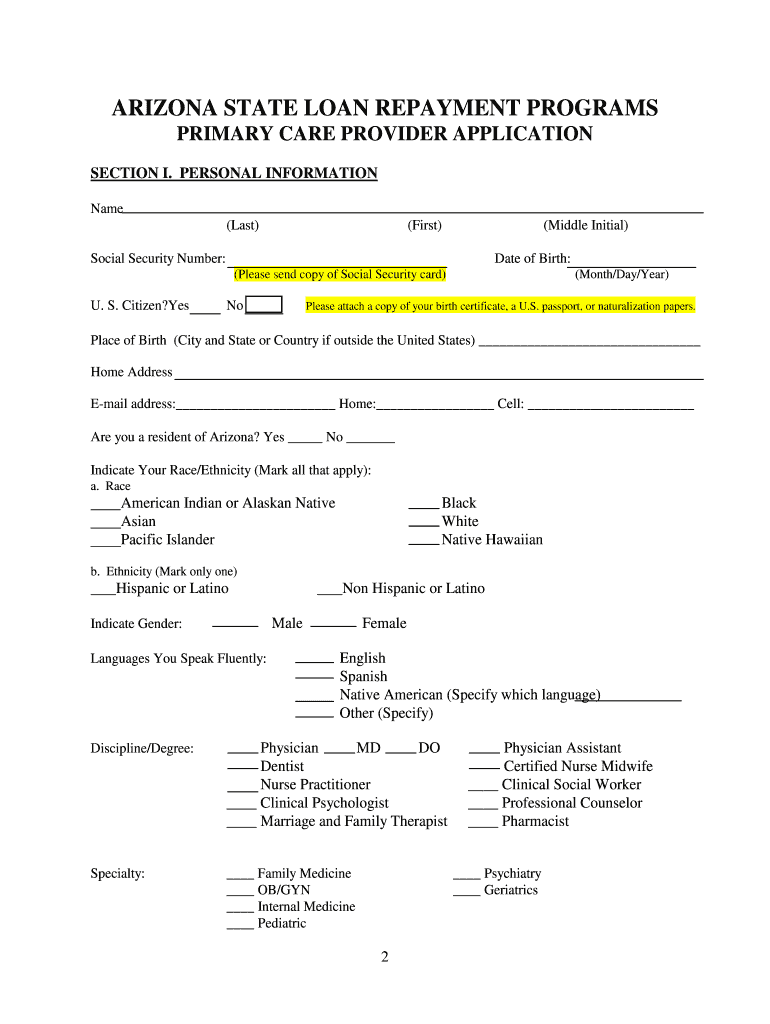
ARIZONA STATE LOAN REPAYMENT PROGRAMS PROVIDER APPLICATION Mail completed Application to: Arizona Department of Health Services Bureau of Health Systems Development Attn: Loan Repayment Program Manager
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign primary care bprovider applicationb
Edit your primary care bprovider applicationb form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your primary care bprovider applicationb form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing primary care bprovider applicationb online



In order to make advantage of the professional PDF editor, follow these steps below:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit primary care bprovider applicationb. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
With pdfFiller, it's always easy to deal with documents.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out primary care bprovider applicationb
How to fill out primary care provider application?
01
Gather all necessary documents and information: Before starting the application, make sure you have all the required documents such as identification proof, medical licenses, certifications, and professional references. Additionally, you will need to provide personal information like your contact details, educational background, and work experience.
02
Research the application process: Familiarize yourself with the specific requirements and guidelines outlined by the primary care provider organization you are applying to. Understanding the application process will help you navigate it more efficiently and ensure you don't miss any important steps.
03
Complete the personal information section: Begin by filling out your personal details including your full name, date of birth, social security number, and current address. Be sure to provide accurate and up-to-date information to avoid any delays in the application process.
04
Include your educational background: Enter your academic qualifications, including the institutions you attended, degrees obtained, and graduation dates. It's essential to provide accurate information regarding your education to demonstrate your qualifications as a primary care provider.
05
Provide your work experience: Indicate your previous work experience in the healthcare field. Include the names of the organizations you have worked for, your job titles, dates of employment, and a brief description of your responsibilities. It is helpful to highlight any relevant experience that showcases your skills and expertise in primary care.
06
List your certifications and licenses: Include any professional certifications and licenses you hold that are relevant to primary care. Provide the issuing authority, certificate/license number, as well as expiration dates if applicable. This section is crucial to demonstrate your compliance with regulatory requirements.
07
Submit professional references: Provide contact information for professional references who can vouch for your capabilities as a primary care provider. Make sure to inform your references in advance, so they are prepared to receive a call or email regarding your application.
08
Check for completeness and accuracy: Double-check all the information you have entered in the application form before submitting it. Review for any spelling errors, missing details, or discrepancies. Accuracy and attention to detail are crucial in creating a favorable impression.
Who needs primary care provider application?
01
Medical professionals seeking employment: Doctors, nurse practitioners, physician assistants, and other healthcare professionals who wish to work in primary care settings need to complete a primary care provider application.
02
Graduating students: Recent medical graduates or those about to complete their medical or healthcare-related degree seeking opportunities in primary care would be required to fill out a provider application.
03
Residents or fellows: Individuals currently participating in residency or fellowship programs and planning to transition into primary care practice may need to complete a provider application as part of their job search process.
04
Healthcare organizations: Some healthcare organizations that provide primary care services may require new providers to complete an application to be considered for employment within their system.
Note: The specifics of who needs a primary care provider application may vary depending on the policies and requirements of the respective institutions or organizations. It is advisable to check with the specific organization you are interested in working with to determine if an application is required.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I execute primary care bprovider applicationb online?
Easy online primary care bprovider applicationb completion using pdfFiller. Also, it allows you to legally eSign your form and change original PDF material. Create a free account and manage documents online.
Can I create an electronic signature for the primary care bprovider applicationb in Chrome?
Yes. With pdfFiller for Chrome, you can eSign documents and utilize the PDF editor all in one spot. Create a legally enforceable eSignature by sketching, typing, or uploading a handwritten signature image. You may eSign your primary care bprovider applicationb in seconds.
How do I complete primary care bprovider applicationb on an Android device?
On an Android device, use the pdfFiller mobile app to finish your primary care bprovider applicationb. The program allows you to execute all necessary document management operations, such as adding, editing, and removing text, signing, annotating, and more. You only need a smartphone and an internet connection.
What is primary care provider application?
Primary care provider application is a form that healthcare professionals need to submit in order to become a primary care provider in a healthcare network or system.
Who is required to file primary care provider application?
Healthcare professionals such as doctors, nurse practitioners, and physician assistants who want to work as primary care providers.
How to fill out primary care provider application?
The application usually requires personal information, medical credentials, work experience, and references to be filled out accurately.
What is the purpose of primary care provider application?
The purpose is to ensure that qualified healthcare professionals are able to provide primary care services to patients in need.
What information must be reported on primary care provider application?
Information such as credentials, work history, references, and any relevant certifications must be reported.
Fill out your primary care bprovider applicationb online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Primary Care Bprovider Applicationb is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
