Centre Dermatology Aesformtic Medicine Patient Medical free printable template
Show details
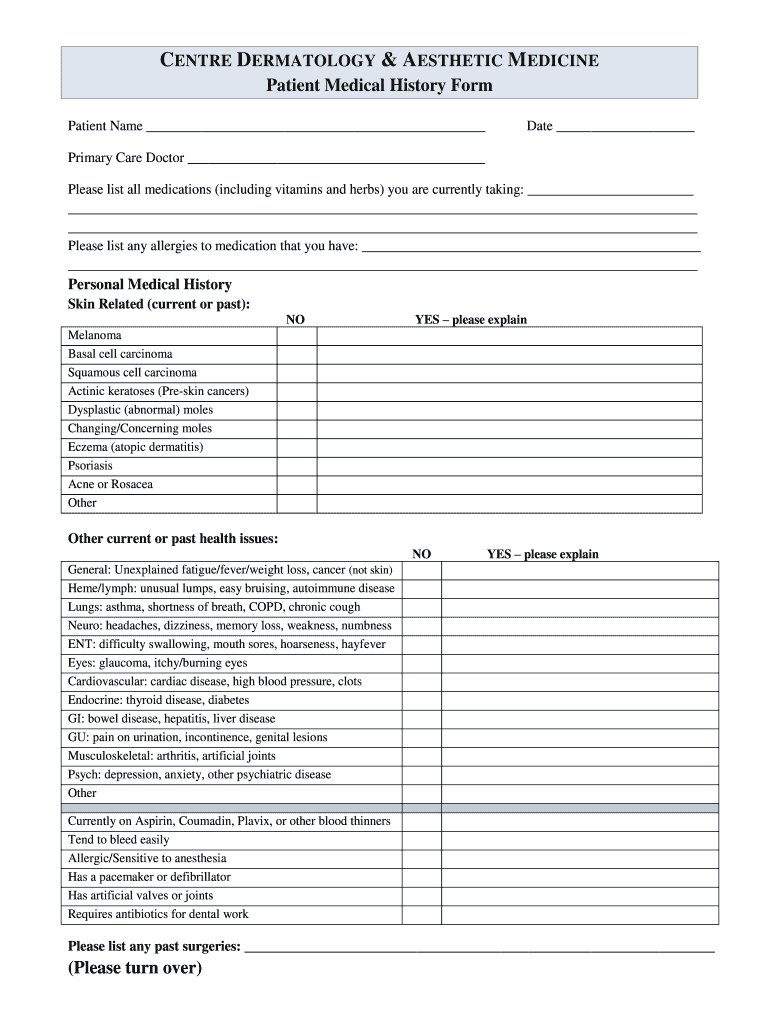
Center DERMATOLOGY & AESTHETIC MEDICINE Patient Medical History Form Patient Name Date Primary Care Doctor Please list all medications (including vitamins and herbs) you are currently taking: Please
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign health history form

Edit your health history form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your health history form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing health history form online



To use our professional PDF editor, follow these steps:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit health history form. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Save your file. Choose it from the list of records. Then, shift the pointer to the right toolbar and select one of the several exporting methods: save it in multiple formats, download it as a PDF, email it, or save it to the cloud.
pdfFiller makes dealing with documents a breeze. Create an account to find out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out health history form

How to fill out a health history form:
01
Start by carefully reading the instructions provided on the form. Make sure you understand what information is required and how to effectively complete each section.
02
Begin by providing accurate personal details such as your full name, date of birth, address, and contact information. This ensures your identity can be verified and allows healthcare providers to easily reach you if needed.
03
Next, provide information about your medical history. This may include previous illnesses, surgeries, chronic conditions, allergies, medication you are currently taking, and any significant medical events in your past. Be thorough and specific, as this information greatly assists healthcare professionals in understanding your medical background.
04
Fill out the section pertaining to your family medical history. Include details about any significant illnesses or conditions that occur within your immediate family, such as heart disease, diabetes, or cancer. These can be important factors in assessing your overall health and potential risk factors.
05
If the form requests information about your lifestyle habits, be honest and provide accurate details. This may include questions about smoking, alcohol consumption, exercise routines, and dietary habits. Your habits can have a significant impact on your overall health, and healthcare professionals need this information to better assess and advise you.
06
If there is a section dedicated to current symptoms or concerns, describe any specific issues you are currently experiencing. Include details about the duration, intensity, and any triggers or alleviating factors you have noticed. This information helps healthcare providers prioritize and address your immediate needs.
Who needs a health history form:
01
Individuals seeking medical care or treatment from any healthcare provider, whether it is a physician, nurse, dentist, or specialist, may be required to fill out a health history form. This form helps the healthcare provider gain a comprehensive understanding of your past and present health, allowing them to make informed decisions and provide personalized care.
02
Insurance companies may also require individuals to complete a health history form when applying for coverage or making a claim. This information helps insurers assess risk and determine appropriate coverage options.
03
Some institutions and organizations, such as schools, sports teams, or employment workplaces, may request a health history form to ensure individuals can safely participate in certain activities. This form helps identify any underlying health conditions or risks that may affect a person's ability to engage in specific activities.
Overall, health history forms are essential tools that gather comprehensive information about an individual's medical background, enabling healthcare providers to deliver appropriate and personalized care.
Fill
form
: Try Risk Free
People Also Ask about
How do I fill out a health history form?
Here are some important areas an effective medical history form should cover: Patient contact information. Age and gender. History of surgeries and treatments. Previous tests and scans. Dates and timeline of symptoms. Family medical history. Past diseases and illnesses. Known allergies.
What is included in a health history form?
In general, a medical history includes an inquiry into the patient's medical history, past surgical history, family medical history, social history, allergies, and medications the patient is taking or may have recently stopped taking.
How do you ask for history of present illness?
History of Present Illness o When did it start / how long has it been going on? o Is this a new problem / first time having this problem? o Intermittent or constant? o What makes it worse • Any other symptoms that you have?
What questions are asked for medical history?
Ask questions like: How old are you? Do you or did anyone in our family have any long-term health problems, like heart disease, diabetes, kidney disease, bleeding disorder, or lung disease? Do you or did anyone in our family have any health issues like high blood pressure, high cholesterol, or asthma?
How do I fill out a health history?
Here are some important areas an effective medical history form should cover: Patient contact information. Age and gender. History of surgeries and treatments. Previous tests and scans. Dates and timeline of symptoms. Family medical history. Past diseases and illnesses. Known allergies.
What 10 components should be included in a health history questionnaire?
Personal status. Family and social relationships. Diet and Nutrition. Functional ability. Mental Health. Personal Habits. Health promotion activities. Environment.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I execute health history form online?
pdfFiller has made filling out and eSigning health history form easy. The solution is equipped with a set of features that enable you to edit and rearrange PDF content, add fillable fields, and eSign the document. Start a free trial to explore all the capabilities of pdfFiller, the ultimate document editing solution.
How can I edit health history form on a smartphone?
You can easily do so with pdfFiller's apps for iOS and Android devices, which can be found at the Apple Store and the Google Play Store, respectively. You can use them to fill out PDFs. We have a website where you can get the app, but you can also get it there. When you install the app, log in, and start editing health history form, you can start right away.
How do I fill out the health history form form on my smartphone?
Use the pdfFiller mobile app to complete and sign health history form on your mobile device. Visit our web page (https://edit-pdf-ios-android.pdffiller.com/) to learn more about our mobile applications, the capabilities you’ll have access to, and the steps to take to get up and running.
What is Centre Dermatology & Aesthetic Medicine Patient Medical?
Centre Dermatology & Aesthetic Medicine Patient Medical is a medical form used by the Centre for documenting the health history, condition, and treatment preferences of patients seeking dermatological and aesthetic services.
Who is required to file Centre Dermatology & Aesthetic Medicine Patient Medical?
All patients seeking services at the Centre Dermatology & Aesthetic Medicine are required to file the Patient Medical form to ensure comprehensive care.
How to fill out Centre Dermatology & Aesthetic Medicine Patient Medical?
To fill out the Patient Medical form, patients should provide accurate personal information, medical history, current conditions, allergies, and any treatments they are undergoing. It is important to complete all sections of the form thoroughly.
What is the purpose of Centre Dermatology & Aesthetic Medicine Patient Medical?
The purpose of the Patient Medical form is to collect essential health information that assists healthcare providers in diagnosing and treating dermatological and aesthetic concerns effectively.
What information must be reported on Centre Dermatology & Aesthetic Medicine Patient Medical?
Patients must report personal identification details, medical history, current medications, allergies, skin concerns, and previous treatments related to dermatology or aesthetics on the Patient Medical form.
Fill out your health history form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Health History Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
