
Get the free PATIENT HEALTH INFORMATION - bNEDLCb
Show details
New England Dermatology & Laser Center 3455 Main Street, Suite 5 Springfield, MA 01107 (413) 7339600 www.nedlc.com COSMETIC CONSULTATION QUESTIONNAIRE Patient Name: Date: Chart#: Gender: M F Age Date
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign patient health information
Edit your patient health information form online
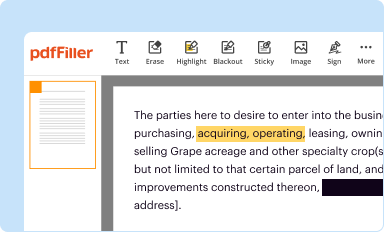
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
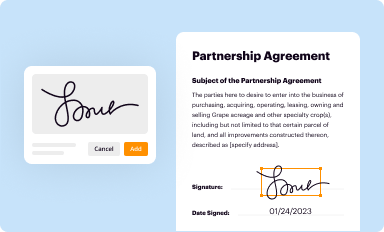
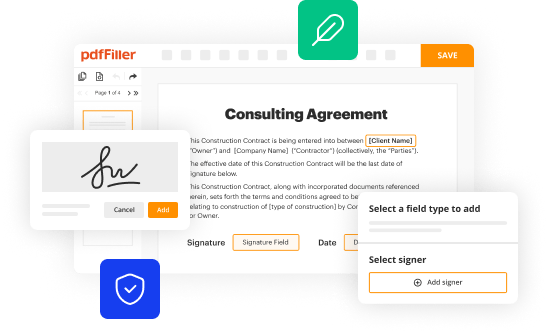
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
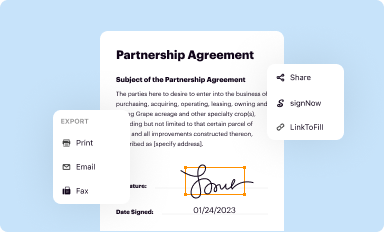
Share your form instantly
Email, fax, or share your patient health information form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing patient health information online



In order to make advantage of the professional PDF editor, follow these steps below:
1
Log into your account. In case you're new, it's time to start your free trial.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit patient health information. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Get your file. Select the name of your file in the docs list and choose your preferred exporting method. You can download it as a PDF, save it in another format, send it by email, or transfer it to the cloud.
With pdfFiller, it's always easy to work with documents. Try it out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out patient health information
How to fill out patient health information:
01
Start by accessing the patient health information form provided by the healthcare provider or institution.
02
Write the patient's full name, including first name, middle name (if applicable), and last name, in the designated space.
03
Enter the patient's date of birth or age, as well as their gender.
04
Provide the patient's contact details, such as their current address, phone number, and email address.
05
Indicate the patient's primary healthcare provider or regular physician, including their name, clinic/hospital name, and contact information.
06
Specify any allergies or adverse reactions the patient may have to medications, food, or other substances. Include details about the severity of these allergies or reactions if necessary.
07
List the current medications the patient is taking, including the name, dosage, and frequency of each medication.
08
Mention any pre-existing medical conditions, chronic illnesses, or disabilities that are relevant to the patient's overall health.
09
Provide information about the patient's medical history, including any past surgeries, hospitalizations, or significant medical events.
10
Include the patient's family medical history, especially if there are hereditary conditions or diseases that run in the family.
11
Endorse any immunizations or vaccinations the patient has received, along with the dates and types of vaccines.
12
If applicable, document the patient's insurance information, including the name of the insurance company, policy number, and any relevant contact details.
13
Sign and date the patient health information form to certify the accuracy and completeness of the provided information.
Who needs patient health information:
01
Healthcare providers: Doctors, nurses, and other healthcare professionals need patient health information to assess and provide appropriate medical care. It helps them make informed decisions, diagnose conditions, and develop treatment plans.
02
Emergency medical personnel: In the case of an emergency or when a patient cannot communicate, having access to their health information is crucial for making quick decisions and providing immediate care.
03
Insurance companies: Patient health information is necessary for insurance companies to process claims, verify medical necessity, and ensure appropriate coverage for healthcare services.
04
Researchers and public health agencies: Health information can be anonymized and used for research or population health studies to improve healthcare practices and outcomes.
05
Legal purposes: Patient health information might be required for legal proceedings, such as disability claims, medical disputes, or personal injury cases.
06
Patients themselves: Having access to their own health information allows patients to track their medical history, stay informed about their conditions and treatments, and participate in their own healthcare decisions.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I make changes in patient health information?
With pdfFiller, the editing process is straightforward. Open your patient health information in the editor, which is highly intuitive and easy to use. There, you’ll be able to blackout, redact, type, and erase text, add images, draw arrows and lines, place sticky notes and text boxes, and much more.
Can I create an eSignature for the patient health information in Gmail?
Use pdfFiller's Gmail add-on to upload, type, or draw a signature. Your patient health information and other papers may be signed using pdfFiller. Register for a free account to preserve signed papers and signatures.
How do I edit patient health information on an Android device?
You can. With the pdfFiller Android app, you can edit, sign, and distribute patient health information from anywhere with an internet connection. Take use of the app's mobile capabilities.
Fill out your patient health information online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Patient Health Information is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
