
Get the free MR ARTHROGRAPHY Patient Information and Consent Form - dzu
Show details
MR ARTHROGRAPHY Patient Information and Consent Form Patients Name: Date: (Please fill out) IF YOU HAVE A CARDIAC PACEMAKER, PLEASE NOTIFY THE STAFF AT THE INFORMING IMMEDIATELY IF YOU MAY BE OR ARE
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign mr arthrography patient information
Edit your mr arthrography patient information form online
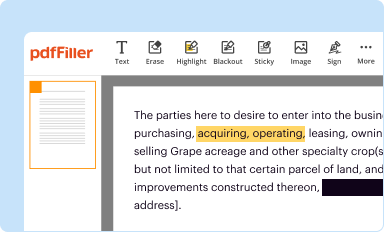
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
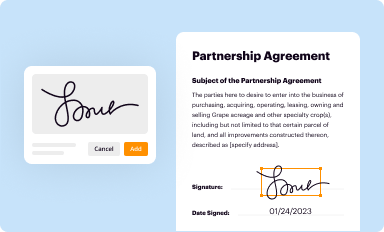
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
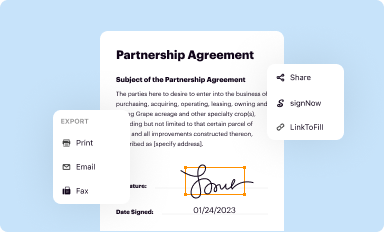
Share your form instantly
Email, fax, or share your mr arthrography patient information form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit mr arthrography patient information online



Follow the guidelines below to benefit from the PDF editor's expertise:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit mr arthrography patient information. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
With pdfFiller, it's always easy to work with documents.
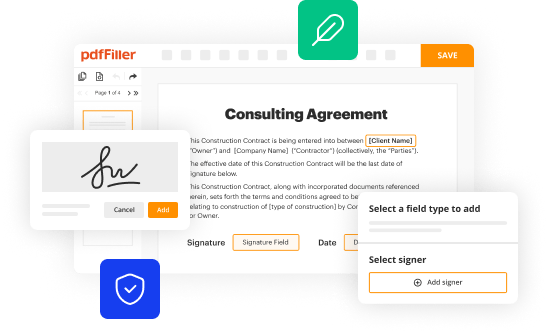
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out mr arthrography patient information
How to fill out MR arthrography patient information:
01
Start by providing personal details such as the patient's full name, date of birth, and contact information. This ensures accurate identification and communication throughout the process.
02
Next, fill in the medical history section. Include any relevant information regarding previous surgeries, allergies, current medications, or any existing medical conditions. This is crucial for the radiologist to assess the risks and plan the procedure accordingly.
03
Make sure to provide a detailed description of the reason for the MR arthrography. Explain any symptoms or concerns that led to the recommendation of this imaging test. This information helps the radiologist to focus on the specific area of interest during the procedure.
04
Specify any previous imaging studies related to the same problem. If the patient has undergone X-rays, CT scans, or previous MRIs in the affected area, provide the details, such as the date and location of the study. This allows the radiologist to compare the current findings with the previous ones for a more accurate diagnosis.
05
Indicate if the patient has any metal implants or devices in their body. Metallic objects, such as pacemakers, stents, or implanted pumps, can interfere with the MR arthrography procedure or cause potential safety issues. Informing the medical staff about these implants helps them take necessary precautions.
06
Lastly, sign and date the patient information form to confirm that all the provided information is accurate and complete. This serves as consent for the procedure and ensures that the patient takes responsibility for the provided details.
Who needs MR arthrography patient information:
01
Patients scheduled to undergo MR arthrography.
02
Orthopedic surgeons or specialists recommending or referring patients for MR arthrography.
03
Radiologists or radiology technologists responsible for performing the MR arthrography procedure.
04
Medical staff involved in the patient's care and treatment, such as nurses or anesthesiologists.
05
Insurance providers or billing departments that require accurate patient information for billing and reimbursement purposes.
06
Research institutions or clinical trials conducting studies related to MR arthrography, which may require the patient information for data collection and analysis.
07
Legal or administrative authorities in case of any medico-legal issues or regulatory requirements.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I edit mr arthrography patient information in Chrome?
Install the pdfFiller Google Chrome Extension to edit mr arthrography patient information and other documents straight from Google search results. When reading documents in Chrome, you may edit them. Create fillable PDFs and update existing PDFs using pdfFiller.
How can I edit mr arthrography patient information on a smartphone?
The easiest way to edit documents on a mobile device is using pdfFiller’s mobile-native apps for iOS and Android. You can download those from the Apple Store and Google Play, respectively. You can learn more about the apps here. Install and log in to the application to start editing mr arthrography patient information.
How do I edit mr arthrography patient information on an Android device?
With the pdfFiller mobile app for Android, you may make modifications to PDF files such as mr arthrography patient information. Documents may be edited, signed, and sent directly from your mobile device. Install the app and you'll be able to manage your documents from anywhere.
Fill out your mr arthrography patient information online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Mr Arthrography Patient Information is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
