Last updated on Mar 31, 2026
Get the free Medication Change Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
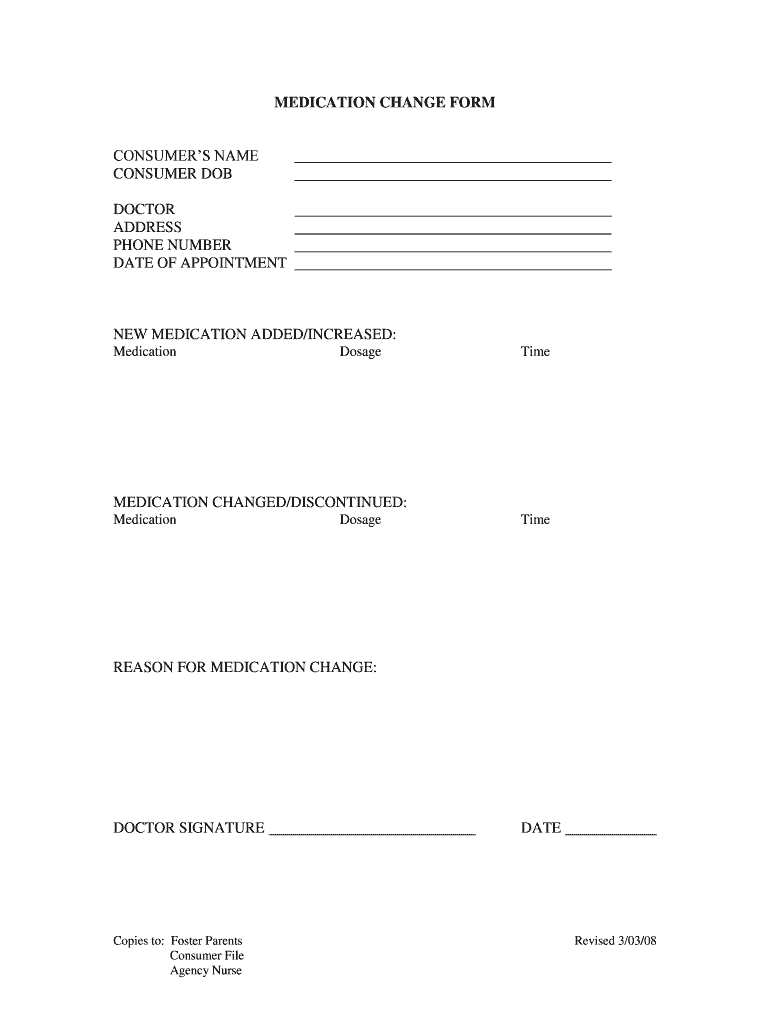
What is medication change form
The Medication Change Form is a medical consent document used by healthcare providers to record changes in a consumer's medication regimen.
pdfFiller scores top ratings on review platforms
Who needs medication change form?
Explore how professionals across industries use pdfFiller.

Medication change form is needed by:
-
Doctors requiring changes in medication for patients
-
Foster parents managing medication for children
-
Agency nurses overseeing health documentation
-
Healthcare administrators handling consent forms
-
Patients needing documented approval for medication adjustments
-
Caregivers involved in medication management
Comprehensive Guide to medication change form
Overview of the Medication Change Form
The Medication Change Form serves a critical role in the healthcare system by documenting adjustments in a patient’s medication regimen. This form is designed to enhance communication between healthcare providers and ensures that all necessary information is accurately recorded. The accuracy of the information on this form is vital, as it requires the doctor's signed consent to confirm their approval for the medication changes.
Using a medical consent form that captures detailed medication adjustments minimizes errors that could affect patient safety. Proper documentation not only protects the patient's well-being but also satisfies regulatory requirements for transparency in healthcare practices.
Purpose and Benefits of the Medication Change Form
The Medication Change Form is indispensable for ensuring clear and accurate documentation of any medication changes. As a healthcare document template, it has significant implications for all stakeholders involved, including patients, their caregivers, and healthcare agencies.
-
Clear documentation helps prevent medical errors during transitions.
-
Patients benefit from a streamlined process for medication management.
-
Healthcare providers are ensured compliance with safety protocols.
Ultimately, the form serves as a safeguard to promote patient safety when medication adjustments are necessary, reaffirming trust among patients and their healthcare providers.
Key Features of the Medication Change Form
This form includes various critical sections that facilitate documentation of medication changes. Important areas feature consumer information, medication tables, and sections requiring the doctor's signature.
-
Consumer details: Name and date of birth are required for identification.
-
Medication tables list new medications added or adjustments made.
-
Doctor's signature area provides accountability for the changes.
-
Copies of the form are distributed to relevant parties for transparency.
Such features underscore the importance of having a comprehensive medication change template that can accommodate the complexities of medication management.
Who Should Use the Medication Change Form?
Eligible users of the Medication Change Form include healthcare providers, patients, and healthcare agencies. This document is particularly essential in scenarios requiring medication adjustments and should always involve the physician's input and approval.
-
Doctors need to complete and sign the form to validate changes.
-
Patients must provide accurate medication history for effective revisions.
-
Agencies may require the form to ensure compliance with care standards.
Recognizing the roles of each user emphasizes the collaborative nature of medication management and reinforces the necessity for accurate documentation.
How to Fill Out the Medication Change Form Online
To effectively complete the Medication Change Form using pdfFiller, follow these key steps for a seamless experience. Collect all necessary information, including patient data and specifics about the medication.
-
Access the Medication Change Form on pdfFiller.
-
Input consumer details, including the patient’s name and date of birth.
-
Incorporate details for any new medications, dosage, and administration time.
-
Ensure the doctor's section is filled out accurately prior to submission.
-
Review the form for accuracy to avoid common mistakes before finalizing.
This step-by-step guide ensures users understand the requirements for correctly filling out the medication change consent.
Submitting and Managing the Medication Change Form
After completing the Medication Change Form, users can choose various submission methods. Understanding the submission process is critical for effective management and follow-up.
-
Forms may be submitted electronically for swift processing.
-
Physical submissions require reliable tracking mechanisms for confirmation.
-
Maintain copies of the submitted form for future reference and accountability.
Effective submission and managing of this healthcare form is essential for ensuring that necessary medication changes are communicated and recorded properly.
Security and Compliance with the Medication Change Form
Handling sensitive information through the Medication Change Form necessitates strict adherence to data security measures. Institutions must ensure that the form complies with relevant regulations, such as HIPAA.
-
Privacy measures are applied to protect patient data throughout the process.
-
pdfFiller employs security features to safeguard document integrity.
-
Consistent training on careful handling of medical records is crucial.
Reinforcing security practices ensures that patient information remains confidential, which is paramount when dealing with sensitive medical documentation.
Real-World Example of a Medication Change Form
Providing a filled-out example of the Medication Change Form can clarify its usage and instructions. A practical illustration can assist users in understanding how to adapt the form for their specific needs.
Common scenarios that necessitate changes, as shown in the example, will illustrate the form’s practical applications and the importance of following the correct protocols.
Harnessing pdfFiller for Your Medication Change Form Needs
Utilizing pdfFiller for creating and managing the Medication Change Form offers numerous advantages, enhancing user experience. The platform allows for easy editing and the incorporation of eSignatures, streamlining the workflow.
-
pdfFiller supports customizable forms, meeting varied user needs.
-
The cloud-based nature allows for access from any browser without downloads.
-
Robust security features ensure compliance while handling sensitive documents.
Users should consider leveraging pdfFiller for their medication management form requirements to capitalize on these benefits.
How to fill out the medication change form
-
1.Visit pdfFiller and log in or create an account if you do not have one.
-
2.Search for the Medication Change Form in the template library or use the upload option if it's not readily available.
-
3.Open the form by clicking on it; this will load it into the pdfFiller editor.
-
4.Review the blank fields at the top of the form, collecting necessary information such as the consumer’s name, date of birth, and doctor's contact details before entering them.
-
5.Use the text boxes provided to fill in information precisely as required, ensuring to carefully document the medication changes including the name, dosage, and timing for each medication.
-
6.Refer to the structured tables for 'NEW MEDICATION ADDED/INCREASED' or 'MEDICATION CHANGED/DISCONTINUED' to input relevant medication information accurately.
-
7.Once you have filled in all required fields, check that the form is complete, and review the entries for any errors or missing information.
-
8.Make sure the doctor’s signature field is clear; you may need to print the form for the doctor to sign if it’s not filled electronically.
-
9.After finalizing the form, use the 'Save' or 'Download' option to store it on your device.
-
10.To submit, review pdfFiller for any direct submission options, or follow your usual procedures for submitting such forms in your healthcare setting.

What are the eligibility requirements to use the Medication Change Form?
The Medication Change Form is typically used by healthcare professionals and authorized caregivers when documenting changes in a consumer's medication. Ensure you have the necessary permissions to make medication changes and that the form is complete before use.
Are there any deadlines for submitting the Medication Change Form?
While specific deadlines vary by agency or healthcare provider, it’s advisable to submit the Medication Change Form as soon as changes occur to ensure proper monitoring and records. Always consult your organization’s guidelines.
What methods can I use to submit the Medication Change Form?
You can submit the Medication Change Form electronically via email or an online portal if available. Alternatively, print the completed form for physical submission. Confirm with your healthcare institution for specific submission protocols.
Are there any required supporting documents for this form?
Typically, supporting documents may include prescriptions, previous medication records, or medical history. Check the specific requirements of your healthcare provider to ensure all necessary documentation accompanies the form.
What common mistakes should I avoid when filling out the Medication Change Form?
Common mistakes include incomplete fields, wrong dosages, or missing the doctor's signature. Always double-check all entries for accuracy and ensure that required sections are filled before submission.
What are the processing times for the Medication Change Form?
Processing times depend on the healthcare provider or agency receiving the form. Some changes may be approved immediately while others might take several days. Be sure to follow up if there are concerns about timing.
What happens if my Medication Change Form is incomplete?
An incomplete Medication Change Form may delay the medication adjustment process or may be rejected outright. Always ensure that all required information is accurately entered and that it is signed by a relevant healthcare professional.
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.