
HHS CMS-1490 (Formerly CMS-1490S) 2005 free printable template
Show details
Patient s employment 4b I Yes B. Accident I Auto 4c I No I Other Was patient being treated with chronic dialysis or kidney transplant a. Are you employed and covered under an employee health plan b. Is your spouse employed and are you covered under your spouse s employee health plan c. If you have any medical coverage other than Medicare such as private insurance employment related insurance State Agency Medicaid or the VA complete Name and Addre...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign HHS CMS-1490 Formerly CMS-1490S
Edit your HHS CMS-1490 Formerly CMS-1490S form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your HHS CMS-1490 Formerly CMS-1490S form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit HHS CMS-1490 Formerly CMS-1490S online



Follow the steps below to benefit from the PDF editor's expertise:
1
Register the account. Begin by clicking Start Free Trial and create a profile if you are a new user.
2
Upload a file. Select Add New on your Dashboard and upload a file from your device or import it from the cloud, online, or internal mail. Then click Edit.
3
Edit HHS CMS-1490 Formerly CMS-1490S. Add and replace text, insert new objects, rearrange pages, add watermarks and page numbers, and more. Click Done when you are finished editing and go to the Documents tab to merge, split, lock or unlock the file.
4
Save your file. Select it from your list of records. Then, move your cursor to the right toolbar and choose one of the exporting options. You can save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud, among other things.
It's easier to work with documents with pdfFiller than you could have believed. You may try it out for yourself by signing up for an account.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
HHS CMS-1490 (Formerly CMS-1490S) Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out HHS CMS-1490 Formerly CMS-1490S
How to fill out HHS CMS-1490 (Formerly CMS-1490S)
01
Obtain the HHS CMS-1490 form from the official HHS website or a local Medicare office.
02
Fill in the beneficiary's information, including their name, Medicare number, and date of birth at the top of the form.
03
Specify the medical service or item for which you are seeking reimbursement in the designated section.
04
Itemize the costs associated with the medical service or item in the appropriate fields.
05
Provide a detailed explanation of your claim, including why the service/item was necessary.
06
Attach any required documentation, such as receipts, invoices, and supporting medical records.
07
Review the form for accuracy and completeness before signing it.
08
Submit the completed form to the appropriate Medicare office either by mail or electronically.
Who needs HHS CMS-1490 (Formerly CMS-1490S)?
01
Individuals who have received medical services or items that are covered by Medicare and wish to seek reimbursement.
02
Beneficiaries who have paid out-of-pocket expenses for eligible medical expenses not billed directly to Medicare.
03
Persons appealing a denial of service by Medicare that requires the submission of the form for reconsideration.
Fill
form
: Try Risk Free
People Also Ask about
What is the first step in submitting Medicare claims?
The first step in submitting a Medicare claim is the health provider must submit the covered expenses.
Can I submit a claim to Medicare myself?
Contact your doctor or supplier, and ask them to file a claim. If they don't file a claim, call us at 1-800-MEDICARE (1-800-633-4227). TTY: 1-877-486-2048.
What is form CMS 1490S?
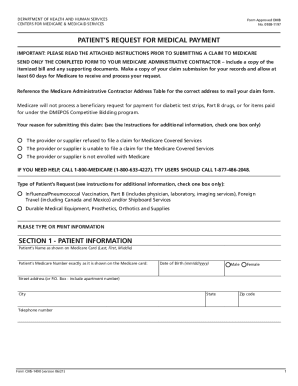
CMS 1490S: Patient's Request For Medical Payment | CMS. An official website of the United States government Here's how you know.
What is a CMS 1490S form?
DEPARTMENT OF HEALTH AND HUMAN SERVICES. CENTERS FOR MEDICARE & MEDICAID SERVICES. Form Approved OMB.
What is a CMS 1450 form used for?
The CMS-1450 form (aka UB-04 at present) can be used by an institutional provider to bill a Medicare fiscal intermediary (FI) when a provider qualifies for a waiver from the Administrative Simplification Compliance Act (ASCA) requirement for electronic submission of claims.
What is the purpose of the standard CMS 1500 claim form?
The CMS-1500 form is the standard claim form used by a non-institutional provider or supplier to bill Medicare carriers and durable medical equipment regional carriers (DMERCs) when a provider qualifies for a waiver from the Administrative Simplification Compliance Act (ASCA) requirement for electronic submission of
What is Medicare Form CMS 1490S?
SEND ONLY THE COMPLETED FORM TO YOUR MEDICARE ADMINISTRATIVE CONTRACTOR – Include a copy of the itemized bill and any supporting documents. Make a copy of your claim submission for your records and allow at least 60 days for Medicare to receive and process your request.
How do I submit a Medicare claim electronically?
How to Submit Medicare Claims Electronically Step 1: Begin EDI Enrollment. EDI enrollment is a necessary first step in getting electronic claims submission processes up and running. Step 2: Notify Your MAC. Step 3: Submit Electronic Healthcare Claims to the MAC. Step 4: Get Reimbursed.
How do I withdraw from Medicare Part B?
You can voluntarily terminate your Medicare Part B (Medical Insurance). However, you may need to have a personal interview with Social Security to review the risks of dropping coverage and to assist you with your request.
How do I fill out the CMS form 1763?
How to fill out Form CMS 1763? Name of Enrollee. Medicare Number. Name of the Person, if Other than Enrollee, Who Is Executing the Request (if appropriate). This is a Request for Termination of Hospital Insurance/Medical Insurance. Date Hospital Insurance Will End. Reasons for the termination request.
What is CMS 1763 for?
The completion of this form is needed to document your voluntary request for termination of Medicare coverage as permitted under the Code of Federal Regulations.
How to fill out a 1500 claim form for Medicare?
How to fill out a CMS-1500 form The type of insurance and the insured's ID number. The patient's full name. The patient's date of birth. The insured's full name, if applicable. The patient's address. The patient's relationship to the insured, if applicable. The insured's address, if applicable. Field reserved for NUCC use.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I fill out the HHS CMS-1490 Formerly CMS-1490S form on my smartphone?
You can easily create and fill out legal forms with the help of the pdfFiller mobile app. Complete and sign HHS CMS-1490 Formerly CMS-1490S and other documents on your mobile device using the application. Visit pdfFiller’s webpage to learn more about the functionalities of the PDF editor.
How do I edit HHS CMS-1490 Formerly CMS-1490S on an iOS device?
Yes, you can. With the pdfFiller mobile app, you can instantly edit, share, and sign HHS CMS-1490 Formerly CMS-1490S on your iOS device. Get it at the Apple Store and install it in seconds. The application is free, but you will have to create an account to purchase a subscription or activate a free trial.
How do I complete HHS CMS-1490 Formerly CMS-1490S on an Android device?
Complete your HHS CMS-1490 Formerly CMS-1490S and other papers on your Android device by using the pdfFiller mobile app. The program includes all of the necessary document management tools, such as editing content, eSigning, annotating, sharing files, and so on. You will be able to view your papers at any time as long as you have an internet connection.
What is HHS CMS-1490 (Formerly CMS-1490S)?
HHS CMS-1490 (formerly CMS-1490S) is a form used by Medicare beneficiaries to report and request reimbursement for medical expenses incurred due to dialysis, including home dialysis.
Who is required to file HHS CMS-1490 (Formerly CMS-1490S)?
Individuals who are Medicare beneficiaries and have incurred out-of-pocket expenses for dialysis services are required to file HHS CMS-1490.
How to fill out HHS CMS-1490 (Formerly CMS-1490S)?
To fill out HHS CMS-1490, individuals must complete the sections identifying their personal information, the details of the incurred expenses, and attach any relevant documentation such as receipts or invoices.
What is the purpose of HHS CMS-1490 (Formerly CMS-1490S)?
The purpose of HHS CMS-1490 is to facilitate the reimbursement process for Medicare beneficiaries for out-of-pocket medical expenses related to dialysis.
What information must be reported on HHS CMS-1490 (Formerly CMS-1490S)?
The information that must be reported on HHS CMS-1490 includes the beneficiary's personal information, type of service received, dates of service, total charges, amounts paid by Medicare, and any other insurance information.
Fill out your HHS CMS-1490 Formerly CMS-1490S online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
HHS CMS-1490 Formerly CMS-1490s is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
