Workers Compensation Case Intake Form 2013-2026 free printable template
Show details
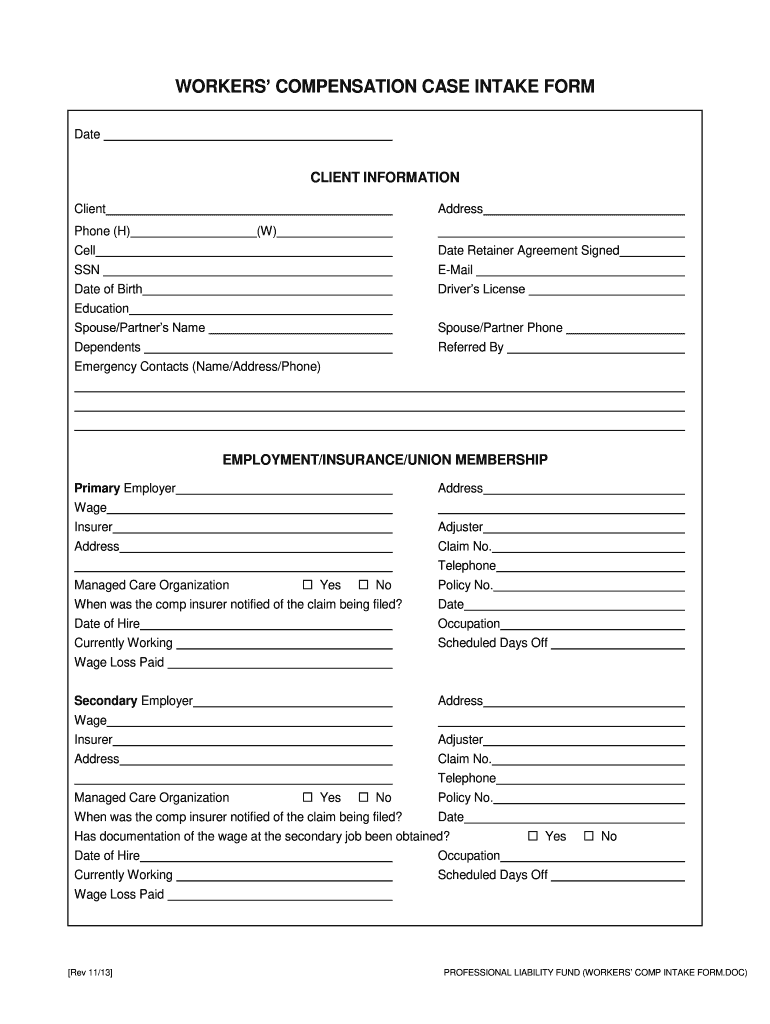
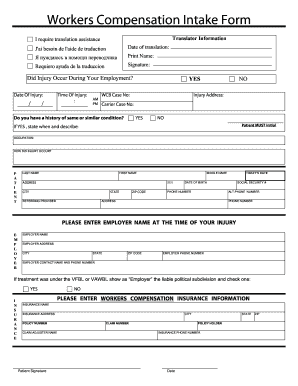
WORKERS COMPENSATION CASE INTAKE FORM Date CLIENT INFORMATION Client Address Phone H W Cell Date Retainer Agreement Signed SSN Date of Birth E-Mail Driver s License Education Spouse/Partner s Name Dependents Referred By Emergency Contacts Name/Address/Phone EMPLOYMENT/INSURANCE/UNION MEMBERSHIP Primary Employer Wage Insurer Adjuster Claim No. Telephone Managed Care Organization Yes No When was the comp insurer notified of the claim being filed Policy No. Date of Hire Currently Working...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign workers comp form pdf
Edit your workers compensation form pdf form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your workers compensation claim form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit workers compensation intake form online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Register the account. Begin by clicking Start Free Trial and create a profile if you are a new user.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit printable workers compensation form. Replace text, adding objects, rearranging pages, and more. Then select the Documents tab to combine, divide, lock or unlock the file.
4
Save your file. Select it from your list of records. Then, move your cursor to the right toolbar and choose one of the exporting options. You can save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud, among other things.
pdfFiller makes dealing with documents a breeze. Create an account to find out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out workers compensation insurance form
How to fill out Workers Compensation Case Intake Form
01
Begin by filling out your personal information, including your name, address, phone number, and email.
02
Provide the details of your employer, including the company's name, address, and contact information.
03
Specify the date and time when the injury occurred.
04
Describe the nature of the injury and how it happened in detail.
05
List any witnesses to the incident, including their names and contact information.
06
Document any medical treatment you have received since the injury.
07
Attach any relevant documents, such as medical records or incident reports.
08
Review the completed form for accuracy before submitting it.
Who needs Workers Compensation Case Intake Form?
01
Employees who have been injured at work and wish to file a claim for workers' compensation.
02
Employers who need to document workplace injuries and initiate claims on behalf of their employees.
03
Legal professionals assisting clients with workers' compensation cases.
Fill
workers comp forms
: Try Risk Free
People Also Ask about workers comp intake form
What is a CA 16 form?
Form CA-16 - Authorization for Examination and/or Treatment. This form guarantees payment to the care provider if the employee requires medical treatment because of a work-related traumatic injury. Your supervisor should complete page 1 of Form CA-16 and provide it to you for your attending physicians information.
What is a CA 2 form used for?
This form is used if the employee has sustained an occupational disease as a result of job duties.
What is the difference between CA1 and CA2 form?
Most work-related medical conditions fall into two categories: (1) traumatic injury (Form CA-1, Federal Employee's Notice of Traumatic Injury and Claim for Continuation of Pay/Compensation), and (2) occupational disease (Form CA-2, Notice of Occupational Disease and Claim for Compensation).
What is a DWC 1 claim form?
A DWC 1 is the form that is filled out to report an injury to your employer, and officially initiate a workers' compensation claim.
What is a CA 17 form?
Injured postal workers are required to fill in form CA-17, which is a form which outlines information from a doctor forbidding an injured federal employee from carrying out certain activities due to their inherently physically taxing nature.
What is a CA 3 form?
REPORT. If the employee is receiving disability compensation periodically each four weeks, the official superior should immediately telephone or telegraph the OWCP advising the date employee returned to work. This will avoid an overpayment of compensation. Follow-up should then be made with Form CA-3.
Our user reviews speak for themselves
Read more or give pdfFiller a try to experience the benefits for yourself
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
Can I sign the workers comp form electronically in Chrome?
Yes. By adding the solution to your Chrome browser, you may use pdfFiller to eSign documents while also enjoying all of the PDF editor's capabilities in one spot. Create a legally enforceable eSignature by sketching, typing, or uploading a photo of your handwritten signature using the extension. Whatever option you select, you'll be able to eSign your workers compensation outline in seconds.
How can I edit workers' compensation form pdf on a smartphone?
Using pdfFiller's mobile-native applications for iOS and Android is the simplest method to edit documents on a mobile device. You may get them from the Apple App Store and Google Play, respectively. More information on the apps may be found here. Install the program and log in to begin editing workers compensation template.
How can I fill out workers compensation paperwork on an iOS device?
Install the pdfFiller iOS app. Log in or create an account to access the solution's editing features. Open your claim form for workers compensation by uploading it from your device or online storage. After filling in all relevant fields and eSigning if required, you may save or distribute the document.
What is Workers Compensation Case Intake Form?
The Workers Compensation Case Intake Form is a document used to collect necessary information from an injured worker, which is essential for initiating a workers' compensation claim.
Who is required to file Workers Compensation Case Intake Form?
Generally, any employee who has sustained a work-related injury or illness must file a Workers Compensation Case Intake Form to initiate a claim for benefits.
How to fill out Workers Compensation Case Intake Form?
To fill out the Workers Compensation Case Intake Form, gather relevant information such as personal details, details of the injury or illness, incident date, treatment received, and any witness information, and ensure all sections of the form are completed accurately.
What is the purpose of Workers Compensation Case Intake Form?
The purpose of the Workers Compensation Case Intake Form is to capture essential information required by insurance companies or employers to process and evaluate claims for workers' compensation benefits.
What information must be reported on Workers Compensation Case Intake Form?
The Workers Compensation Case Intake Form typically requires information such as the injured worker's name, contact information, work details, description of the injury, medical treatment sought, and any relevant witness information.
Fill out your Workers Compensation Case Intake Form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Wc Form is not the form you're looking for?Search for another form here.
Keywords relevant to comp form
Related to workers compensation documents




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
