
Get the free PROVIDER NOMINATION FORM Please complete this form if you ...
Show details
Suite 150 Rancho Cordova CA 95670 Fax 916 852-2380 Your Name Date Company Name of Provider Ophthalmologist MD Optometrist OD Optician or Optical Store Street Address City State Zip Code Email address Telephone Fax If you have any questions regarding a provider nomination please call Customer Service at 800 507-3800. Please note that every effort will be made to consider your nomination. However geographical network space provider s response or Superior Vision s qualifying guidelines may...
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign provider nomination form please
Edit your provider nomination form please form online
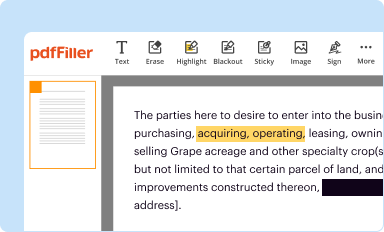
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
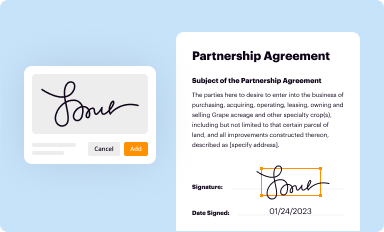
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
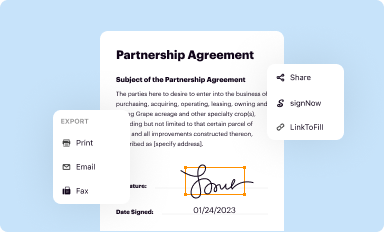
Share your form instantly
Email, fax, or share your provider nomination form please form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit provider nomination form please online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit provider nomination form please. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
Dealing with documents is simple using pdfFiller. Try it right now!
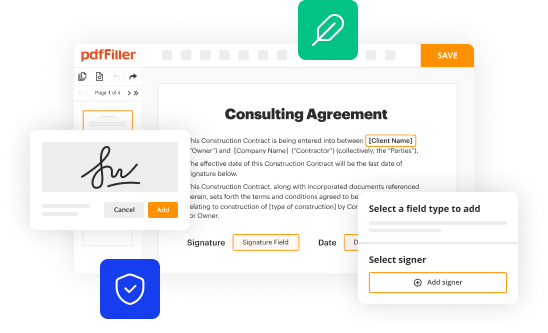
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out provider nomination form please
How to fill out provider nomination form please
01
To fill out the provider nomination form, follow these steps:
02
Start by accessing the provider nomination form online or obtain a physical copy from the relevant organization.
03
Read the instructions carefully to understand the requirements and eligibility criteria for nominating a provider.
04
Begin by entering your personal details such as your name, contact information, and any affiliation you may have with the organization.
05
Provide the name and relevant details of the provider you wish to nominate, such as their organization, contact information, and specialty.
06
Include a short description explaining why you believe this provider should be nominated and their qualifications for the nomination.
07
If required, attach any supporting documents that validate the provider's achievements, contributions, or qualifications.
08
Review the filled form to ensure all information is accurate and complete.
09
Submit the form as per the instructions provided. If submitting online, click the submit button. If submitting a physical copy, deliver it to the designated location.
10
Keep a copy of the filled form for your records.
11
Wait for confirmation or further communication from the organization regarding the status of your nomination.
Who needs provider nomination form please?
01
The provider nomination form is typically needed by individuals or organizations who want to nominate a specific healthcare provider for recognition, awards, or other forms of acknowledgment.
02
This form is commonly used by patients, colleagues, healthcare professionals, or administrators who have knowledge of a healthcare provider's exceptional skills, contributions, or achievements.
03
Organizations, including medical associations, hospitals, clinics, or health committees, may also require the provider nomination form to facilitate the process of selecting and recognizing outstanding providers.
04
By completing this form, the nominator puts forward a recommendation for a provider's recognition, helping to bring attention to their dedication and excellence in the healthcare field.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I edit provider nomination form please from Google Drive?
pdfFiller and Google Docs can be used together to make your documents easier to work with and to make fillable forms right in your Google Drive. The integration will let you make, change, and sign documents, like provider nomination form please, without leaving Google Drive. Add pdfFiller's features to Google Drive, and you'll be able to do more with your paperwork on any internet-connected device.
How can I get provider nomination form please?
The premium pdfFiller subscription gives you access to over 25M fillable templates that you can download, fill out, print, and sign. The library has state-specific provider nomination form please and other forms. Find the template you need and change it using powerful tools.
How do I edit provider nomination form please on an Android device?
You can edit, sign, and distribute provider nomination form please on your mobile device from anywhere using the pdfFiller mobile app for Android; all you need is an internet connection. Download the app and begin streamlining your document workflow from anywhere.
What is provider nomination form please?
Provider nomination form is a form used to nominate a healthcare provider to participate in a specific healthcare plan or network.
Who is required to file provider nomination form please?
Healthcare providers or their authorized representatives are required to file the provider nomination form.
How to fill out provider nomination form please?
The provider nomination form can be filled out online or in paper form, and typically requires information about the provider's qualifications and contact details.
What is the purpose of provider nomination form please?
The purpose of the provider nomination form is to ensure that qualified healthcare providers are included in a specific healthcare plan or network.
What information must be reported on provider nomination form please?
The provider nomination form typically requires information such as the provider's name, contact information, qualifications, specialties, and any relevant certifications.
Fill out your provider nomination form please online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Provider Nomination Form Please is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
