
Get the free Patient Medical History Form - 2015.docx
Show details
Please b ring a list if possible Allergies to m edications If so what medications Do you use cigarettes/tobacco alcohol or other substances following health problems Allergies Arthritis Blood/Lymph Bronchitis Cancer Cholesterol Digestive Ears/Nose/Throat Endocrine Eczema/Rashes Fatigue Fevers Genitourinary High Blood Pressure Integumentary Skin Kidney Muscle/Bone Neurological Psychological Respiratory Sinus Throat Infections Thyroid Unusual weight...
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign patient medical history form
Edit your patient medical history form form online
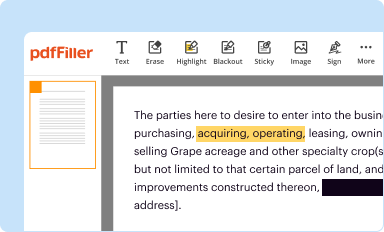
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
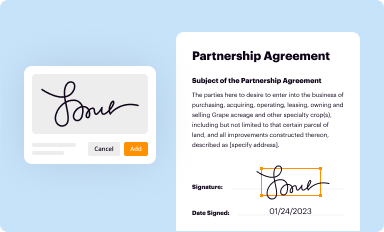
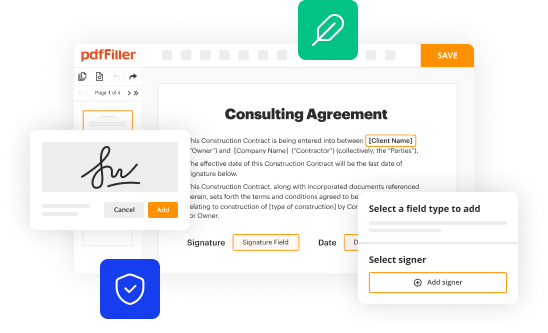
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
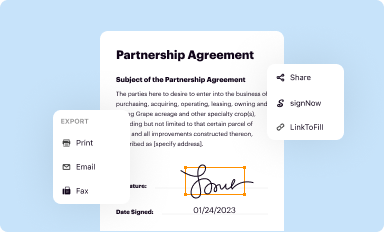
Share your form instantly
Email, fax, or share your patient medical history form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit patient medical history form online



To use the services of a skilled PDF editor, follow these steps below:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit patient medical history form. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Get your file. Select the name of your file in the docs list and choose your preferred exporting method. You can download it as a PDF, save it in another format, send it by email, or transfer it to the cloud.
pdfFiller makes dealing with documents a breeze. Create an account to find out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out patient medical history form
How to fill out patient medical history form
01
Read the instructions carefully before starting to fill out the form.
02
Provide accurate and complete information about the patient's personal details such as name, date of birth, and contact information.
03
Include information about past medical conditions, surgeries, and hospitalizations.
04
Mention any current medications, allergies, or adverse reactions to medications.
05
Document the patient's family medical history, including any hereditary diseases or conditions.
06
Provide details about the patient's lifestyle factors such as smoking, alcohol consumption, and exercise habits.
07
Include information about any ongoing treatments or therapies the patient is undergoing.
08
Make sure to sign and date the form to validate the information provided.
Who needs patient medical history form?
01
Healthcare providers such as doctors, nurses, and medical specialists need patient medical history forms to assess and understand the patient's overall health status.
02
Hospitals, clinics, and healthcare facilities require patient medical history forms for record-keeping and to provide appropriate treatment and care.
03
Insurance companies may request patient medical history forms to evaluate insurance applications and determine coverage.
04
Researchers and scientists might use patient medical history forms for studying and analyzing health trends and patterns.
05
Patients themselves may need to fill out medical history forms when switching healthcare providers or undergoing new medical procedures.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I send patient medical history form for eSignature?
When you're ready to share your patient medical history form, you can swiftly email it to others and receive the eSigned document back. You may send your PDF through email, fax, text message, or USPS mail, or you can notarize it online. All of this may be done without ever leaving your account.
How do I edit patient medical history form online?
With pdfFiller, it's easy to make changes. Open your patient medical history form in the editor, which is very easy to use and understand. When you go there, you'll be able to black out and change text, write and erase, add images, draw lines, arrows, and more. You can also add sticky notes and text boxes.
How do I fill out patient medical history form using my mobile device?
Use the pdfFiller mobile app to complete and sign patient medical history form on your mobile device. Visit our web page (https://edit-pdf-ios-android.pdffiller.com/) to learn more about our mobile applications, the capabilities you’ll have access to, and the steps to take to get up and running.
What is patient medical history form?
Patient medical history form is a document that contains information about a patient's past and current medical conditions, treatments, surgeries, allergies, and medications.
Who is required to file patient medical history form?
Patients are usually required to fill out and file their own medical history form, but in some cases, healthcare providers or caregivers may assist.
How to fill out patient medical history form?
To fill out a patient medical history form, individuals need to provide accurate and detailed information about their medical history, including any past illnesses, surgeries, medications, allergies, and family history of diseases.
What is the purpose of patient medical history form?
The purpose of patient medical history form is to provide healthcare providers with essential information about a patient's health status, which can help guide treatment decisions and improve patient outcomes.
What information must be reported on patient medical history form?
Information that must be reported on patient medical history form includes past and current medical conditions, surgeries, medications, allergies, family history of diseases, and lifestyle habits.
Fill out your patient medical history form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Patient Medical History Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
