
Get the free PATIENT INFORMATION FORMS 1/2015
Show details
Goffman M. D. 8588 Katy Frwy 101 Houston Texas 77024 Advance Notice of Non-covered Charges Medical and Vision insurance does not cover all services. Cardiovascular Gastrointestinal Immunologic High Blood Pressure Hepatitis Sjogren s Syndrome Neurological Vertigo Acid Reflux Sarcoidosis Migraines Cancer- Colon Shingles Mitral Valve Prolapse Cancer- Liver Cold Sores/Fever Blisters Headaches Heart Disease Tuberculosis Constitutional Good General Health Genitourinary Menopause Integumentary/Skin...
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign patient information forms 12015
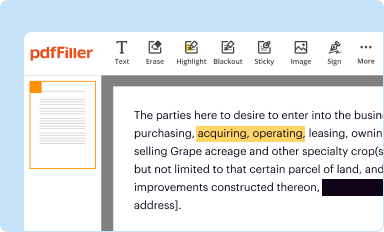
Edit your patient information forms 12015 form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
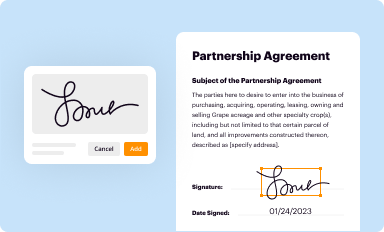
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
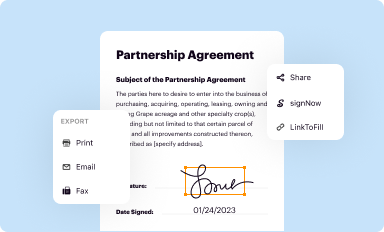
Share your form instantly
Email, fax, or share your patient information forms 12015 form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing patient information forms 12015 online



In order to make advantage of the professional PDF editor, follow these steps below:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit patient information forms 12015. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
Dealing with documents is always simple with pdfFiller. Try it right now
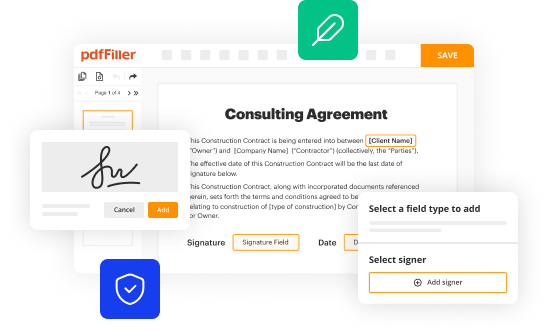
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out patient information forms 12015
How to fill out patient information forms 12015
01
Open the patient information form 12015.
02
Start by filling out the basic information section including the patient's name, date of birth, and contact details.
03
Move on to the medical history section and provide accurate and complete information about the patient's past and current medical conditions, allergies, medications, and surgeries.
04
Fill out the insurance information section, including the insurance provider's name, policy number, and any other relevant details.
05
If applicable, provide details about the patient's primary care physician or referring physician.
06
Complete any additional sections or fields required by the specific form 12015, such as emergency contacts or consent forms.
07
Review the filled information form for any errors or missing information.
08
Sign and date the form if required.
09
Submit the completed patient information form to the relevant healthcare provider or organization.
Who needs patient information forms 12015?
01
Patients who are visiting a healthcare provider for the first time.
02
Patients who are changing their healthcare provider.
03
Patients who need to update their existing medical records.
04
Patients who are participating in clinical trials or research studies.
05
Patients who are applying for health insurance coverage.
06
Patients who are seeking specialized medical treatments.
07
Patients who are undergoing surgical procedures.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I send patient information forms 12015 for eSignature?
Once you are ready to share your patient information forms 12015, you can easily send it to others and get the eSigned document back just as quickly. Share your PDF by email, fax, text message, or USPS mail, or notarize it online. You can do all of this without ever leaving your account.
How do I make edits in patient information forms 12015 without leaving Chrome?
Install the pdfFiller Google Chrome Extension in your web browser to begin editing patient information forms 12015 and other documents right from a Google search page. When you examine your documents in Chrome, you may make changes to them. With pdfFiller, you can create fillable documents and update existing PDFs from any internet-connected device.
Can I create an electronic signature for the patient information forms 12015 in Chrome?
You can. With pdfFiller, you get a strong e-signature solution built right into your Chrome browser. Using our addon, you may produce a legally enforceable eSignature by typing, sketching, or photographing it. Choose your preferred method and eSign in minutes.
What is patient information forms 1?
Patient information forms 1 are documents used to collect and record information about a patient's medical history, personal details, and insurance information.
Who is required to file patient information forms 1?
Healthcare providers, hospitals, clinics, and other medical facilities are required to file patient information forms 1 for each patient they treat or provide services to.
How to fill out patient information forms 1?
Patient information forms 1 can be filled out manually by the patient or electronically through an online portal provided by the healthcare facility. Patients need to provide accurate information about their medical history, current health conditions, contact information, and insurance details.
What is the purpose of patient information forms 1?
The purpose of patient information forms 1 is to collect essential information that healthcare providers need to assess a patient's health status, provide appropriate treatment, and ensure proper billing and insurance processing.
What information must be reported on patient information forms 1?
Patient information forms 1 typically include details such as patient's name, date of birth, address, contact information, medical history, current health conditions, insurance coverage, emergency contacts, and consent for treatment.
Fill out your patient information forms 12015 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Patient Information Forms 12015 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
