Get the free REQUEST FOR bMEDICAL RECORDSbbRELEASEb OF INFORMATION bb
Show details
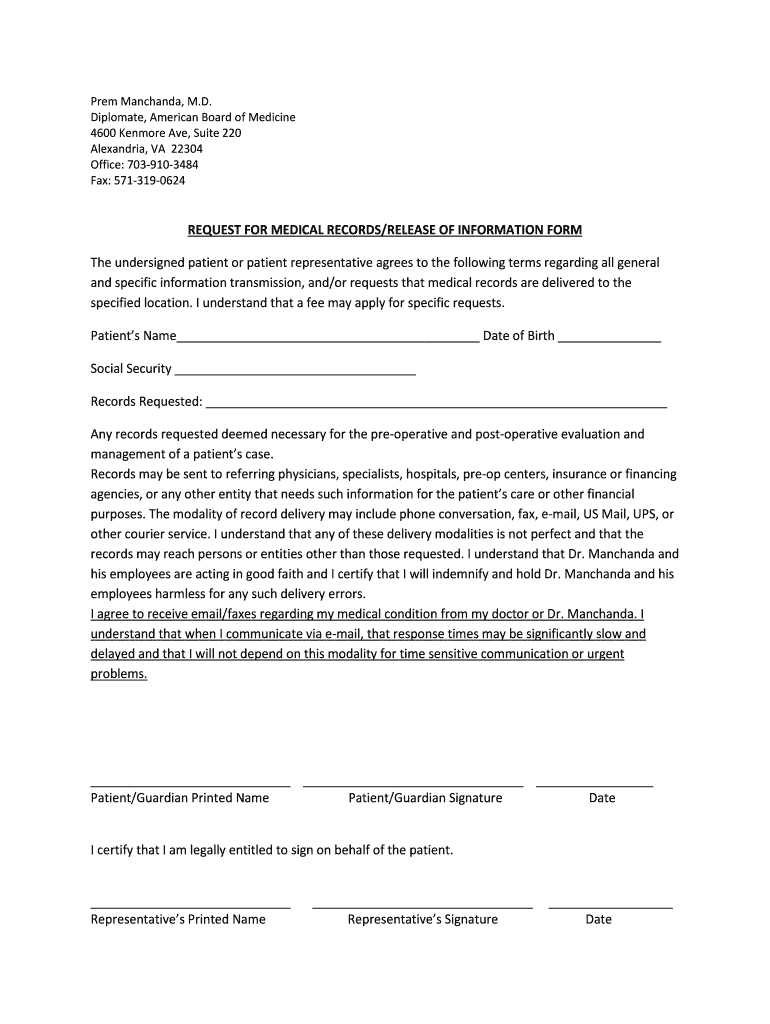
Poem Manchuria, M.D. Diplomat, American Board of Medicine 4600 Kenmore Ave, Suite 220 Alexandria, VA 22304 Office: 7039103484 Fax: 5713190624 REQUEST FOR MEDICAL RECORDS/RELEASE OF INFORMATION FORM
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign request for bmedical recordsbbreleaseb
Edit your request for bmedical recordsbbreleaseb form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your request for bmedical recordsbbreleaseb form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing request for bmedical recordsbbreleaseb online



In order to make advantage of the professional PDF editor, follow these steps:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit request for bmedical recordsbbreleaseb. Add and change text, add new objects, move pages, add watermarks and page numbers, and more. Then click Done when you're done editing and go to the Documents tab to merge or split the file. If you want to lock or unlock the file, click the lock or unlock button.
4
Save your file. Choose it from the list of records. Then, shift the pointer to the right toolbar and select one of the several exporting methods: save it in multiple formats, download it as a PDF, email it, or save it to the cloud.
pdfFiller makes working with documents easier than you could ever imagine. Create an account to find out for yourself how it works!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out request for bmedical recordsbbreleaseb
How to fill out a request for medical records release?
01
Start by contacting the healthcare provider: Reach out to the healthcare provider from whom you wish to obtain your medical records. This can be a hospital, doctor's office, or any other medical facility. Inquire about their specific process for requesting medical records.
02
Obtain the necessary forms: Most healthcare providers have specific forms that need to be filled out in order to request medical records release. These forms can usually be found on the provider's website or by contacting their medical records department. If not available online, ask if they can mail or email the forms to you.
03
Provide personal information: Fill out the required personal information on the request form. This typically includes your full name, date of birth, address, contact number, and any other identifying information requested. Make sure to provide accurate and up-to-date information to avoid any delays in processing your request.
04
Specify the time period and scope of records: Indicate the specific time frame or date range for the records you are requesting. This can be as specific as certain dates or a general range like "all records from January 2010 to present." Specify whether you want the complete medical records or just specific documents, such as lab results or surgical reports.
05
Choose the method of delivery: Decide how you would like to receive your medical records. Options may include picking up the records in person, having them mailed to you, or receiving them electronically via secure email or online portal. Choose the method that is most convenient and secure for you.
06
Sign and date the form: Read through the entire request form carefully, ensuring that you have filled out all the necessary fields. Sign and date the form in the designated space to authorize the release of your medical records. Failure to provide a signature may result in your request being rejected.
Who needs a request for medical records release?
01
Patients seeking continuity of care: When changing healthcare providers or seeking a second opinion, having access to your complete medical history can be crucial for the new provider to understand your medical background and provide appropriate care.
02
Legal purposes: Attorneys and law firms often require medical records for cases involving personal injury, medical malpractice, or disability claims. Medical records can provide supporting evidence or help in evaluating the extent of injuries.
03
Insurance claims: If you are filing an insurance claim related to a medical condition or accident, your insurance provider may require medical records to validate the claim and determine the appropriate coverage.
04
Researchers and academics: Medical researchers and academicians may request medical records for study purposes, clinical trials, or to enhance medical knowledge and advancements in healthcare.
05
Personal record-keeping: Some individuals may request their medical records for personal record-keeping, better understanding their medical history, or monitoring their own health progress.
Note: It is important to check the specific requirements and laws regarding medical records release in your country or jurisdiction, as they may vary. The process and regulations can also differ depending on the healthcare provider or facility.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I complete request for bmedical recordsbbreleaseb online?
pdfFiller makes it easy to finish and sign request for bmedical recordsbbreleaseb online. It lets you make changes to original PDF content, highlight, black out, erase, and write text anywhere on a page, legally eSign your form, and more, all from one place. Create a free account and use the web to keep track of professional documents.
Can I create an electronic signature for the request for bmedical recordsbbreleaseb in Chrome?
Yes. By adding the solution to your Chrome browser, you can use pdfFiller to eSign documents and enjoy all of the features of the PDF editor in one place. Use the extension to create a legally-binding eSignature by drawing it, typing it, or uploading a picture of your handwritten signature. Whatever you choose, you will be able to eSign your request for bmedical recordsbbreleaseb in seconds.
How do I edit request for bmedical recordsbbreleaseb on an iOS device?
Create, modify, and share request for bmedical recordsbbreleaseb using the pdfFiller iOS app. Easy to install from the Apple Store. You may sign up for a free trial and then purchase a membership.
What is request for medical records release?
A request for medical records release is a formal document that allows an individual to request copies of their medical records from a healthcare provider or facility.
Who is required to file request for medical records release?
The patient or their legal representative is typically required to file a request for medical records release.
How to fill out request for medical records release?
To fill out a request for medical records release, you may need to provide basic information such as your name, date of birth, the name of the healthcare provider or facility, the dates of treatment, and your signature.
What is the purpose of request for medical records release?
The purpose of a request for medical records release is to obtain a copy of your medical records for personal use, to share with another healthcare provider, for insurance claims, or for legal purposes.
What information must be reported on request for medical records release?
The information that must be reported on a request for medical records release typically includes personal information such as name and date of birth, specifics about the medical records being requested, and the purpose for the request.
Fill out your request for bmedical recordsbbreleaseb online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Request For Bmedical Recordsbbreleaseb is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
