
Get the free Physician Information Form
Show details
Any incomplete or misstatements could result in denial of credentialing. I also authorize HAP to access physician information from the Council of Affordable Quality Healthcare ProView database. Complete the information below and sign the form. Return form with a completed W-9 form. Physician Assistant and Nurse Practitioner Only Submit evidence of collaborative or supervision agreemement between applicant and a designated Health Alliance Plan credentialed physician. Name of supervising...
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign physician information form
Edit your physician information form form online
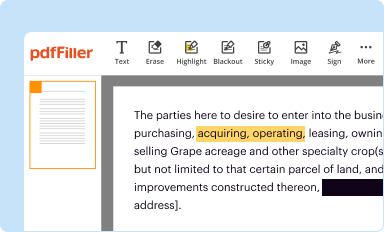
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
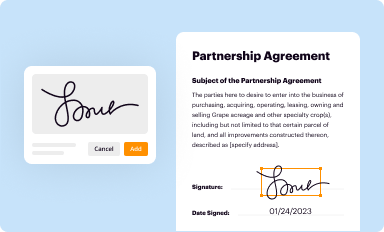
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
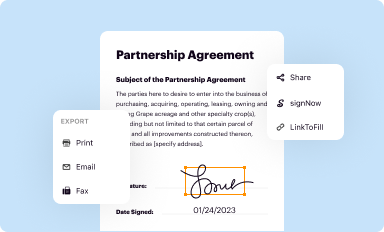
Share your form instantly
Email, fax, or share your physician information form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit physician information form online



To use our professional PDF editor, follow these steps:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit physician information form. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Save your file. Select it from your list of records. Then, move your cursor to the right toolbar and choose one of the exporting options. You can save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud, among other things.
With pdfFiller, it's always easy to work with documents. Check it out!
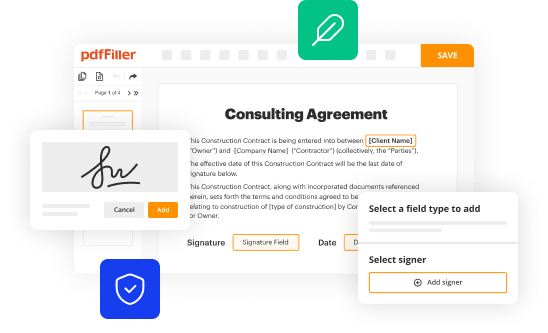
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out physician information form
How to fill out physician information form
01
Read the instructions: Start by carefully reading the instructions accompanying the physician information form. This will provide you with a clear understanding of what information needs to be provided and how it should be filled out.
02
Gather necessary documents: Collect all relevant documents such as medical certifications, licenses, and any other supporting paperwork required by the form.
03
Complete personal information: Begin by providing your personal information such as your full name, contact details, and professional identification numbers.
04
Fill in education and training: Provide detailed information about your medical education, including the name of the medical school, years attended, and any specialized training or residency programs completed.
05
Include professional experience: List your work experience in chronological order, starting with the most recent. Provide information about the name and location of the organization, your position, and the duration of employment.
06
Record certifications and licenses: Clearly document all your certifications and licenses relevant to your medical practice. Include the issuing authority, license number, and expiration date.
07
Submit additional documentation: If required, attach copies of supporting documents such as malpractice insurance, professional references, or any other relevant paperwork.
08
Review and proofread: Before submitting the form, carefully review all the provided information for accuracy and completeness. Make sure to double-check spellings, dates, and contact details.
09
Submit the form: Once you are satisfied with the information provided, submit the completed physician information form through the designated method outlined in the instructions.
10
Follow up: If necessary, follow up with the organization or institution to confirm receipt of the form and to inquire about any additional steps or requirements.
Who needs physician information form?
01
Medical professionals: Physicians, doctors, and other healthcare professionals who are required to provide their information to licensing boards, medical institutions, or regulatory bodies.
02
Medical students: Individuals currently enrolled in medical school or pursuing medical education who need to fill out physician information forms for application or registration purposes.
03
Residents and fellows: Medical residents and fellows who are transitioning to new positions or programs may be required to complete physician information forms as part of the onboarding process.
04
Healthcare organizations: Hospitals, clinics, and healthcare facilities that employ or contract with physicians often require them to fill out physician information forms to ensure compliance with regulatory standards and to maintain accurate records.
05
Licensing boards: State or regional licensing boards that govern the practice of medicine may require physicians to submit updated information through physician information forms to ensure their eligibility to practice.
06
Insurance companies: Insurance providers may require physicians to complete physician information forms to determine their eligibility for participation in insurance networks and to process claims effectively.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I send physician information form for eSignature?
When you're ready to share your physician information form, you can swiftly email it to others and receive the eSigned document back. You may send your PDF through email, fax, text message, or USPS mail, or you can notarize it online. All of this may be done without ever leaving your account.
How do I complete physician information form online?
pdfFiller makes it easy to finish and sign physician information form online. It lets you make changes to original PDF content, highlight, black out, erase, and write text anywhere on a page, legally eSign your form, and more, all from one place. Create a free account and use the web to keep track of professional documents.
How do I fill out physician information form on an Android device?
Complete your physician information form and other papers on your Android device by using the pdfFiller mobile app. The program includes all of the necessary document management tools, such as editing content, eSigning, annotating, sharing files, and so on. You will be able to view your papers at any time as long as you have an internet connection.
What is physician information form?
The physician information form is a document used to collect details about a physician's background, qualifications, and contact information.
Who is required to file physician information form?
Physicians and medical professionals are required to file the physician information form.
How to fill out physician information form?
To fill out the physician information form, the physician must provide accurate and up-to-date information about their education, licensure, work experience, and contact details.
What is the purpose of physician information form?
The purpose of the physician information form is to ensure that all healthcare providers have current and accurate information about licensed physicians.
What information must be reported on physician information form?
Information such as the physician's full name, medical license number, education, work history, and contact information must be reported on the physician information form.
Fill out your physician information form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Physician Information Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
