PR Triple-S Advantage Patients Request for Medical Payment 2017 free printable template
Show details
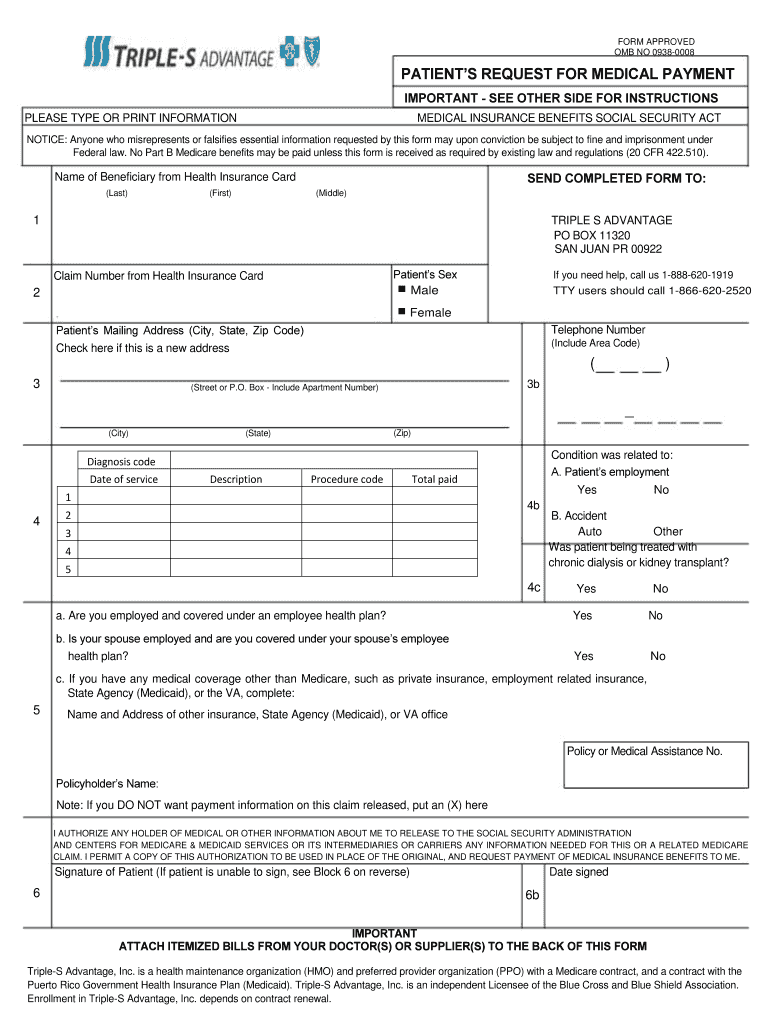
FORM APPROVED OMB NO 09380008PATIENTS REQUEST FOR MEDICAL PAYMENT IMPORTANT SEE OTHER SIDE FOR INSTRUCTIONS PLEASE TYPE OR PRINT INFORMATIONMEDICAL INSURANCE BENEFITS SOCIAL SECURITY NOTICE: Anyone
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign omb no 0938-0008

Edit your omb no 0938-0008 form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your omb no 0938-0008 form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit omb no 0938-0008 online



In order to make advantage of the professional PDF editor, follow these steps:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit omb no 0938-0008. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Get your file. When you find your file in the docs list, click on its name and choose how you want to save it. To get the PDF, you can save it, send an email with it, or move it to the cloud.
With pdfFiller, it's always easy to work with documents. Try it out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
PR Triple-S Advantage Patients Request for Medical Payment Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out omb no 0938-0008

How to fill out PR Triple-S Advantage Patients Request for Medical Payment
01
Obtain the PR Triple-S Advantage Patients Request for Medical Payment form from the official website or customer service.
02
Fill in your personal information at the top of the form, including your name, address, policy number, and contact details.
03
Provide the dates of service for the medical care you are requesting payment for.
04
Enter the provider's information, including their name, address, and license number, if applicable.
05
Specify the type of service received, along with any relevant procedure codes or descriptions.
06
Attach all necessary documentation, such as receipts, bills, and any medical records that support your claim.
07
Review the completed form and documentation for accuracy and completeness.
08
Sign and date the form to certify that the information provided is true and correct.
09
Submit the completed form, along with attachments, to the designated address or fax number provided by the insurance company.
Who needs PR Triple-S Advantage Patients Request for Medical Payment?
01
Patients who are enrolled in the PR Triple-S Advantage health plan and have received medical services.
02
Individuals seeking reimbursement for out-of-pocket medical expenses incurred during treatment.
03
Members who require payment for services not directly billed to the insurance company.
Fill
form
: Try Risk Free
People Also Ask about
How do I submit a claim directly to Medicare?
Contact your doctor or supplier, and ask them to file a claim. If they don't file a claim, call us at 1-800-MEDICARE (1-800-633-4227). TTY: 1-877-486-2048.
How to fill claim form part A?
You can proceed to fill out part A of the form by entering a few primary details of yours, including your full name, policy number, residential address, phone number, and e-mail id. Then, you may need to provide the details of your medical history and hospitalisation.
How to fill out a 1500 claim form?
How to fill out a CMS-1500 form The type of insurance and the insured's ID number. The patient's full name. The patient's date of birth. The insured's full name, if applicable. The patient's address. The patient's relationship to the insured, if applicable. The insured's address, if applicable. Field reserved for NUCC use.
What is the purpose of a health insurance claim form?
A claim form is the document that tells your insurance company more details about the accident or illness in question. This will help them determine if the expenses you are claiming for are covered under your insurance plan or not, so the more information on this form the better.
What patient address is included on the claim form?
Enter the complete address of the patient's place of residence at the time of service. Be sure to use your overseas APO/FPO mailing address. Using a local U.S. address will result in payment problems.
What is a health insurance claim form used for?
Filing a health insurance claim means you're requesting reimbursement or direct payment for medical services that you've already received. The way to obtain benefits or payment is by submitting a claim via a specific form or request. There are two ways to submit your health insurance claim.
How do I submit my Medicare claim electronically?
How to Submit Medicare Claims Electronically Step 1: Begin EDI Enrollment. EDI enrollment is a necessary first step in getting electronic claims submission processes up and running. Step 2: Notify Your MAC. Step 3: Submit Electronic Healthcare Claims to the MAC. Step 4: Get Reimbursed. Extra Steps.
What is Block 12 on the CMS 1500 form?
12. PATIENT'S OR AUTHORIZED PERSON'S SIGNATURE I authorize the release of any medical or other information necessary to process this claim. I also request payment of government benefits either to myself or to the party who accepts assignment below.
What is a OMB 0938 1197 form 1500?
Medicare Administrative Contractors use the data collected on the CMS-1500 and the CMS-1490S to determine the proper amount of reimbursement for Part B medical and other health services (as listed in section 1861(s) of the Social Security Act) provided by physicians and suppliers to beneficiaries.
Can I submit a claim to Medicare myself?
Contact your doctor or supplier, and ask them to file a claim. If they don't file a claim, call us at 1-800-MEDICARE (1-800-633-4227). TTY: 1-877-486-2048.
What is the current version of the Form 02 12 OMB control number?
The revised form is version 02/12, OMB control number 0938-1197. The revised form will replace the previous version of the form 08/05, OMB control number 0938-0999.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I modify omb no 0938-0008 without leaving Google Drive?
pdfFiller and Google Docs can be used together to make your documents easier to work with and to make fillable forms right in your Google Drive. The integration will let you make, change, and sign documents, like omb no 0938-0008, without leaving Google Drive. Add pdfFiller's features to Google Drive, and you'll be able to do more with your paperwork on any internet-connected device.
How can I get omb no 0938-0008?
The premium subscription for pdfFiller provides you with access to an extensive library of fillable forms (over 25M fillable templates) that you can download, fill out, print, and sign. You won’t have any trouble finding state-specific omb no 0938-0008 and other forms in the library. Find the template you need and customize it using advanced editing functionalities.
How do I edit omb no 0938-0008 on an iOS device?
You certainly can. You can quickly edit, distribute, and sign omb no 0938-0008 on your iOS device with the pdfFiller mobile app. Purchase it from the Apple Store and install it in seconds. The program is free, but in order to purchase a subscription or activate a free trial, you must first establish an account.
What is PR Triple-S Advantage Patients Request for Medical Payment?
PR Triple-S Advantage Patients Request for Medical Payment is a form used by patients to request payment for medical services rendered under the Triple-S Advantage insurance plan in Puerto Rico.
Who is required to file PR Triple-S Advantage Patients Request for Medical Payment?
Typically, the patient or their authorized representative is required to file the PR Triple-S Advantage Patients Request for Medical Payment.
How to fill out PR Triple-S Advantage Patients Request for Medical Payment?
To fill out the PR Triple-S Advantage Patients Request for Medical Payment, individuals must provide accurate patient information, details about the medical services received, and any relevant billing information as required by the form.
What is the purpose of PR Triple-S Advantage Patients Request for Medical Payment?
The purpose of the PR Triple-S Advantage Patients Request for Medical Payment is to facilitate the reimbursement process for patients who have incurred medical expenses covered by the Triple-S Advantage plan.
What information must be reported on PR Triple-S Advantage Patients Request for Medical Payment?
Information that must be reported includes the patient's personal information, the details of the medical services provided, provider information, dates of service, and the total amount billed.
Fill out your omb no 0938-0008 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Omb No 0938-0008 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms








If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
