
Get the free Application Medical financial assistance program (mfap) - fairfaxcounty
Show details
FAIRFAX COUNTY, VIRGINIA CONSOLIDATED COMMUNITY FUNDING POOL FY 2015 FY 2016 WORKING TOGETHER FUNDING APPLICATION PACKAGE for July 1, 2014, June 30, 2016, RFP# 2000000828 REQUEST FOR PROPOSAL FAIRFAX
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign application medical financial assistance
Edit your application medical financial assistance form online
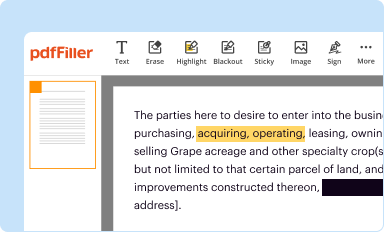
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
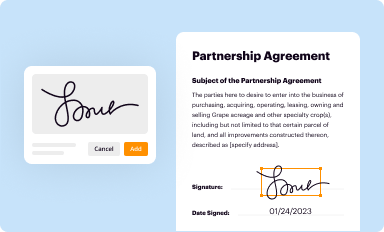
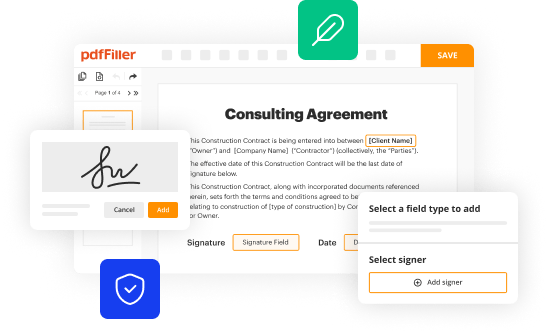
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
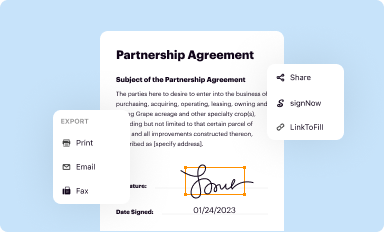
Share your form instantly
Email, fax, or share your application medical financial assistance form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing application medical financial assistance online



Use the instructions below to start using our professional PDF editor:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Upload a file. Select Add New on your Dashboard and upload a file from your device or import it from the cloud, online, or internal mail. Then click Edit.
3
Edit application medical financial assistance. Replace text, adding objects, rearranging pages, and more. Then select the Documents tab to combine, divide, lock or unlock the file.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
pdfFiller makes dealing with documents a breeze. Create an account to find out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out application medical financial assistance
How to fill out application for medical financial assistance:
01
Gather necessary documents: Before starting the application, make sure you have all the required documents such as proof of income, medical bills, and any relevant insurance information.
02
Read the instructions carefully: Review the instructions provided with the application form thoroughly. Pay attention to any specific requirements or documentation needed to complete the application accurately.
03
Provide personal information: Start by filling out personal details such as your name, address, contact information, and social security number. Ensure the information provided is accurate and up to date.
04
Explain the reason for applying: In this section, clearly state the reasons why you are seeking medical financial assistance. Describe your medical condition or situation, and provide any necessary documentation or supporting evidence to strengthen your case.
05
Income and financial information: Provide detailed information about your income, including any employment or government assistance received. Additionally, disclose any assets or savings you might have, as this could impact your eligibility for financial assistance.
06
List medical expenses: Include all medical bills and expenses incurred as a result of your condition. This could include doctor's visits, hospital stays, surgeries, medication costs, and any other related expenses. Make sure you attach copies of the bills or invoices to support your claims.
07
Submit supporting documents: Along with the application form, attach any required supporting documents as specified in the instructions. This might include tax returns, pay stubs, medical records, insurance papers, and proof of residency.
08
Double-check for accuracy: Before submitting the application, go through each section carefully to ensure that all information provided is accurate and complete. Any incorrect or missing information could delay the processing of your application.
09
Follow submission guidelines: Make sure you understand how and where to submit your completed application. Keep a copy of the application form and all supporting documents for your records.
Who needs application for medical financial assistance?
01
Individuals with insufficient health insurance coverage: Those who do not have adequate health insurance coverage or face high deductibles may need to apply for medical financial assistance to help alleviate the burden of medical costs.
02
Low-income individuals or families: Individuals or families with limited income may require medical financial assistance to cover medical expenses that are beyond their financial means.
03
Uninsured or underinsured individuals: People who are either uninsured or have insurance that does not fully cover their medical expenses might need to seek medical financial assistance to access necessary healthcare services.
04
Individuals facing significant medical expenses: Patients who are burdened with substantial medical bills due to chronic illnesses, surgeries, or specialized treatments may benefit from applying for medical financial assistance to lessen the financial strain.
Remember, the specific eligibility criteria and requirements for medical financial assistance may vary depending on the organization or program providing the assistance. It is important to research and reach out to public or private assistance programs in your area to understand their specific application process and requirements.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is application medical financial assistance?
Application medical financial assistance is a form that individuals can fill out to request help with medical expenses.
Who is required to file application medical financial assistance?
Individuals who need financial help with medical expenses are required to file application medical financial assistance.
How to fill out application medical financial assistance?
To fill out application medical financial assistance, individuals must provide personal information, income details, and information about medical expenses.
What is the purpose of application medical financial assistance?
The purpose of application medical financial assistance is to help individuals cover their medical expenses if they are unable to afford them.
What information must be reported on application medical financial assistance?
Information such as personal details, income, and medical expenses must be reported on application medical financial assistance.
How can I modify application medical financial assistance without leaving Google Drive?
People who need to keep track of documents and fill out forms quickly can connect PDF Filler to their Google Docs account. This means that they can make, edit, and sign documents right from their Google Drive. Make your application medical financial assistance into a fillable form that you can manage and sign from any internet-connected device with this add-on.
Can I sign the application medical financial assistance electronically in Chrome?
You certainly can. You get not just a feature-rich PDF editor and fillable form builder with pdfFiller, but also a robust e-signature solution that you can add right to your Chrome browser. You may use our addon to produce a legally enforceable eSignature by typing, sketching, or photographing your signature with your webcam. Choose your preferred method and eSign your application medical financial assistance in minutes.
How do I complete application medical financial assistance on an Android device?
On Android, use the pdfFiller mobile app to finish your application medical financial assistance. Adding, editing, deleting text, signing, annotating, and more are all available with the app. All you need is a smartphone and internet.
Fill out your application medical financial assistance online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Application Medical Financial Assistance is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
