
CA Alameda Alliance for Health Medication Request Form 2013-2025 free printable template
Show details
Alameda Alliance for Health
Medication Request Form
Attn: Prior Authorization Department
200 Stevens Drive
Philadelphia, PA 19113
Phone (Medical/Group Care): 1-855-508-1713
Phone (AllianceSELECT):
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign california alameda alliance health form
Edit your alameda alliance prior authorization form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your ca alameda alliance health form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing alameda alliance form online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Register the account. Begin by clicking Start Free Trial and create a profile if you are a new user.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit alameda alliance medication form. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Save your file. Select it in the list of your records. Then, move the cursor to the right toolbar and choose one of the available exporting methods: save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud.
With pdfFiller, it's always easy to work with documents.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out alameda medication form
How to fill out CA Alameda Alliance for Health Medication Request Form
01
Obtain the CA Alameda Alliance for Health Medication Request Form from the official website or your healthcare provider.
02
Fill in the patient's personal information, including name, date of birth, and member ID.
03
Provide the prescribing physician's details, including name, contact information, and NPI number.
04
Specify the medication requested, including the name, dosage, frequency, and duration of therapy.
05
Include a description of the medical necessity for the medication, such as diagnosis and treatment history.
06
Attach any relevant medical records or documents that support the request.
07
Review the completed form for accuracy and completeness.
08
Sign and date the form, and ensure that the physician also signs it if required.
09
Submit the form as instructed, either by fax or through the online portal, as appropriate.
Who needs CA Alameda Alliance for Health Medication Request Form?
01
Members of the CA Alameda Alliance for Health who require medication that needs prior authorization.
02
Healthcare providers submitting medication requests on behalf of their patients.
03
Patients with specific medical conditions requiring medications not typically covered without prior approval.
Fill
formulary medically
: Try Risk Free
People Also Ask about medication formulary medically
How do I get a new Alameda Alliance card?
If you do not get your Alliance Member ID card after a few weeks of enrolling, or if your card is damaged, lost or stolen, you can: Order a new card online by filling out the Replace ID Card form. Call Member Services at the Alliance to request a new one.
How do I contact Alameda Alliance for Health?
Call your prospective doctor or clinic, medical group, independent practice association, or call Alameda Alliance for Health at 510.747. 4567 to ensure that you can obtain the health care services that you need.
What is the maximum income to qualify for Medi-Cal 2023?
In 2023, the MMNA in CA is $3,715.50 / month. If a non-applicant's monthly income is under this amount, income can be transferred to them from their applicant spouse to bring their income up to $3,715.50.
What is the phone number for Alameda Alliance provider?
2021 PROVIDER DIRECTORY If you have a question about the availability of a provider please call Member Services at 510.747. 4567 or 1.877. 932.2738.
What is the income limit for Medi-Cal in Alameda County?
Beginning July 1, 2022, the asset limit for Non-Modified Adjusted Gross Income (Non-MAGI) Medi-Cal programs increased to $130,000 for a household of one person and $195,000 for a household of two people.
Is Alameda Alliance the same as Medi-Cal?
Welcome to the Alliance! Thank you for joining Alameda Alliance for Health (Alliance). The Alliance is a health plan for people who have Medi-Cal. The Alliance works with the State of California to help you get the health care you need.
What is the maximum income to qualify for Medi-Cal assistance in CA?
ing to Covered California income guidelines and salary restrictions, if an individual makes less than $47,520 per year or if a family of four earns wages less than $97,200 per year, then they qualify for government assistance based on their income.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I modify prescription medication medically without leaving Google Drive?
Simplify your document workflows and create fillable forms right in Google Drive by integrating pdfFiller with Google Docs. The integration will allow you to create, modify, and eSign documents, including ons promotes, without leaving Google Drive. Add pdfFiller’s functionalities to Google Drive and manage your paperwork more efficiently on any internet-connected device.
How do I make changes in formulary hypertension medically?
The editing procedure is simple with pdfFiller. Open your 855 508 1713 in the editor, which is quite user-friendly. You may use it to blackout, redact, write, and erase text, add photos, draw arrows and lines, set sticky notes and text boxes, and much more.
How do I fill out prescription drugs medically on an Android device?
Complete your conditions medically and other papers on your Android device by using the pdfFiller mobile app. The program includes all of the necessary document management tools, such as editing content, eSigning, annotating, sharing files, and so on. You will be able to view your papers at any time as long as you have an internet connection.
What is CA Alameda Alliance for Health Medication Request Form?
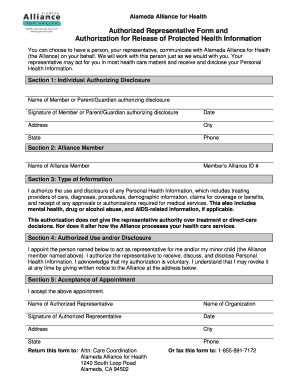
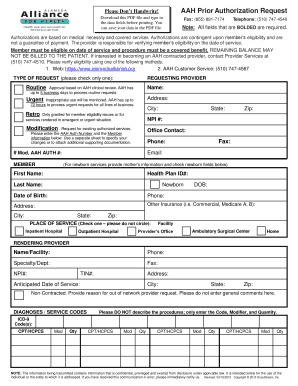
The CA Alameda Alliance for Health Medication Request Form is a document used by healthcare providers to request authorization for specific medications that may not be covered under a patient's insurance plan without prior approval.
Who is required to file CA Alameda Alliance for Health Medication Request Form?
Healthcare providers or prescribers are required to file the CA Alameda Alliance for Health Medication Request Form on behalf of their patients when seeking prior authorization for medications.
How to fill out CA Alameda Alliance for Health Medication Request Form?
To fill out the CA Alameda Alliance for Health Medication Request Form, the provider must include patient information, medication details, clinical rationale for the request, supporting documentation, and provider contact information.
What is the purpose of CA Alameda Alliance for Health Medication Request Form?
The purpose of the CA Alameda Alliance for Health Medication Request Form is to ensure that medications prescribed to patients are medically necessary and appropriate, while also confirming coverage under the patient's insurance plan.
What information must be reported on CA Alameda Alliance for Health Medication Request Form?
The form must report patient demographics, medication name and dosage, diagnosis, previous treatment history, and any relevant medical documentation supporting the request for the medication.
Fill out your alameda alliance authorization form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Alameda Medication Request is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
