
MI BCBS Clinical Editing Appeal Form 2019 free printable template
Show details
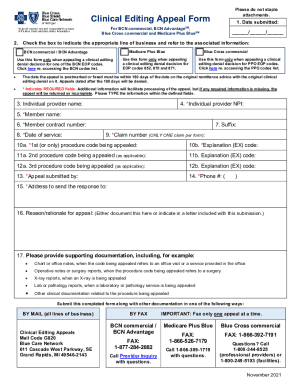
Please do not staple attachments. Clinical Editing Appeal Form1. Date submitted:For BCN HM OSM (commercial), BCN Advantages Blue Cross PPO (commercial) and Blue Cross Medicare Plus Blues PPO / / 2.
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign MI BCBS Clinical Editing Appeal Form

Edit your MI BCBS Clinical Editing Appeal Form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your MI BCBS Clinical Editing Appeal Form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing MI BCBS Clinical Editing Appeal Form online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit MI BCBS Clinical Editing Appeal Form. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Get your file. Select the name of your file in the docs list and choose your preferred exporting method. You can download it as a PDF, save it in another format, send it by email, or transfer it to the cloud.
With pdfFiller, it's always easy to work with documents.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
MI BCBS Clinical Editing Appeal Form Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out MI BCBS Clinical Editing Appeal Form

How to fill out MI BCBS Clinical Editing Appeal Form
01
Obtain the MI BCBS Clinical Editing Appeal Form from the official Michigan BCBS website.
02
Fill in the patient's name and member ID at the top of the form.
03
Provide the date of service and service codes related to the claim being appealed.
04
Briefly describe the reason for the appeal, including any relevant clinical information.
05
Attach supporting documentation, such as medical records or previous correspondence.
06
Review the completed form for accuracy and completeness.
07
Sign and date the form to certify that the information provided is true and correct.
08
Submit the completed form and attachments to the address specified on the form.
Who needs MI BCBS Clinical Editing Appeal Form?
01
Healthcare providers or practitioners who have had a claim denied or adjusted by MI BCBS due to clinical editing.
02
Patients who wish to appeal a decision made by MI BCBS regarding coverage of services rendered.
Fill
form
: Try Risk Free
People Also Ask about
What is the CPT code for prior authorization?
When the trial is rendered in a setting other than the OPD, providers will need to request prior authorization for CPT code 63650 as part of the permanent implantation procedure in the hospital OPD.
What is the timely filing limit for Premera Blue Cross appeal?
Timely Claims Submission Ideally, we'd like you to submit claims within 60 calendar days of the covered services, but no later than 365 calendar days. For most plans, we'll deny claims received more than 12 months after the date of service with no member responsibility.
How do I get authorization from BCBS of Michigan?
Other ways to submit a request Calling 1-800-437-3803. Faxing BCBSM at 1-866-601-4425. Faxing BCN at 1-877-442-3778. Writing: Blue Cross Blue Shield of Michigan, Pharmacy Services. Mail Code 512. Detroit, MI 48226-2998.
Does Michigan Medicaid require prior authorization?
Medicaid requires prior authorization (PA) to cover certain services before those services are rendered to the beneficiary. The purpose of PA is to review the medical need for certain services. It does not serve as an authorization of fees or beneficiary eligibility.
Does BCBS Michigan require prior authorization?
BCBSM requires prior authorization for services or procedures that may be experimental, not always medically necessary, or over utilized. Providers must submit clinical documentation in writing explaining why the proposed procedure or service is medically necessary.
What is the phone number for Blue Cross Blue Shield of Michigan prior authorization?
3. How do providers initiate a prior authorization request? Call 1-877-917-2583 (BLUE) or fax 1-844-407-5293. Hours are 8 a.m. to 7 p.m. Eastern time on weekdays; and 10 a.m. to 5 p.m. on weekends and holidays.
What is the timely filing limit for Blue Care Network of Michigan appeal?
You have 180 days from the date of discovery of a problem to file a grievance with, or appeal a decision of, Blue Cross Blue Shield of Michigan.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I modify my MI BCBS Clinical Editing Appeal Form in Gmail?
In your inbox, you may use pdfFiller's add-on for Gmail to generate, modify, fill out, and eSign your MI BCBS Clinical Editing Appeal Form and any other papers you receive, all without leaving the program. Install pdfFiller for Gmail from the Google Workspace Marketplace by visiting this link. Take away the need for time-consuming procedures and handle your papers and eSignatures with ease.
How can I get MI BCBS Clinical Editing Appeal Form?
The pdfFiller premium subscription gives you access to a large library of fillable forms (over 25 million fillable templates) that you can download, fill out, print, and sign. In the library, you'll have no problem discovering state-specific MI BCBS Clinical Editing Appeal Form and other forms. Find the template you want and tweak it with powerful editing tools.
How do I fill out MI BCBS Clinical Editing Appeal Form using my mobile device?
On your mobile device, use the pdfFiller mobile app to complete and sign MI BCBS Clinical Editing Appeal Form. Visit our website (https://edit-pdf-ios-android.pdffiller.com/) to discover more about our mobile applications, the features you'll have access to, and how to get started.
What is MI BCBS Clinical Editing Appeal Form?
The MI BCBS Clinical Editing Appeal Form is a document used by healthcare providers to contest clinical editing decisions made by Michigan Blue Cross Blue Shield related to claims.
Who is required to file MI BCBS Clinical Editing Appeal Form?
Healthcare providers who wish to appeal a clinical editing determination made by Michigan Blue Cross Blue Shield regarding a claim are required to file this form.
How to fill out MI BCBS Clinical Editing Appeal Form?
To fill out the MI BCBS Clinical Editing Appeal Form, providers should complete all necessary sections including patient information, details of the claim, and a clear explanation of the appeal reasons, and submit it as instructed.
What is the purpose of MI BCBS Clinical Editing Appeal Form?
The purpose of the MI BCBS Clinical Editing Appeal Form is to provide a structured process for healthcare providers to formally challenge and seek reconsideration of clinical editing decisions made on submitted claims.
What information must be reported on MI BCBS Clinical Editing Appeal Form?
The form must include the provider's details, patient's information, claim number, dates of service, specific clinical editing denial reason, and any supporting documentation or comments relevant to the appeal.
Fill out your MI BCBS Clinical Editing Appeal Form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
MI BCBS Clinical Editing Appeal Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
