
NY DOH-5003 2018 free printable template
Show details
Check if verbal consent Leave signature line blank SIGNATURE DATE/TIME PRINT NAME OF DECISION-MAKER PRINT FIRST WITNESS NAME Who made the decisions PRINT SECOND WITNESS NAME Patient Health Care Agent Public Health Law Surrogate Minor s Parent/Guardian Physician or Nurse Practitioner Signature for Sections A and B PHYSICIAN OR NURSE PRACTITIONER SIGNATURE PRINT PHYSICIAN OR NURSE PRACTITIONER NAME 1750-b Surrogate Advance Directives Check all advance directives known to have been completed...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign NY DOH-5003
Edit your NY DOH-5003 form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your NY DOH-5003 form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing NY DOH-5003 online



To use the services of a skilled PDF editor, follow these steps:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit NY DOH-5003. Add and change text, add new objects, move pages, add watermarks and page numbers, and more. Then click Done when you're done editing and go to the Documents tab to merge or split the file. If you want to lock or unlock the file, click the lock or unlock button.
4
Save your file. Select it from your list of records. Then, move your cursor to the right toolbar and choose one of the exporting options. You can save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud, among other things.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
NY DOH-5003 Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out NY DOH-5003
How to fill out NY DOH-5003
01
Obtain the NY DOH-5003 form from the New York State Department of Health website or your local health department.
02
Provide your personal information including your full name, address, and contact details in the designated sections.
03
Indicate the purpose for submitting the form by selecting the appropriate option.
04
Fill out any additional required sections based on the purpose, such as details about the incident or event.
05
Review the form for accuracy, ensuring all information is complete and correct.
06
Sign and date the form at the bottom to validate your submission.
07
Submit the completed form via the indicated method, whether by mail or electronically if applicable.
Who needs NY DOH-5003?
01
Individuals or organizations that are required to report certain health information to the New York State Department of Health.
02
Healthcare providers needing to document public health concerns or incidents.
03
Employers who must report occupational injuries or illnesses.
Fill
form
: Try Risk Free
People Also Ask about
What is medical orders for scope of treatment most?
MOST stands for: Medical Orders for Scope of Treatment. In an emergency or urgent situation, if you are unable to express your wishes, a MOST will help ensure your health care treatment aligns with your wishes.
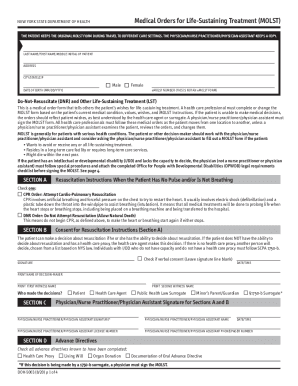
What is the purpose of a MOLST form?
The MOLST form is a set of medical orders for patients with advanced illness who might die within 1-2 years; require long-term care services; or wish to avoid and/or receive specific life-sustaining treatments now. Best practice is to offer MOLST.
What is a MOLST form in NY?
The MOLST form is one way of documenting a patient's treatment preferences concerning life-sustaining treatment – providers may choose to use other forms. However, under State law, the MOLST form is the only authorized form in New York State for documenting both nonhospital DNR and DNI orders.
What is a MOLST in MA?
Massachusetts Medical Orders for Life-Sustaining Treatment (MOLST) is a medical order form (similar to a prescription) that relays instructions between health professionals about a patient's care. MOLST is based on an individual's right to accept or refuse medical treatment, including treatments that might extend life.
Who can fill out a most form?
The MOST Form is for adults over 19 years of age who have a chronic or declining health condition. Ask your MRP if this would be appropriate for you. Once you have a MOST Form it will be reviewed with you as your health changes. A MOST Form may also be completed if you are admitted into a hospital for any reason.
What is the difference between a MOLST and a DNR?
The primary differences between the MOLST form and a DNR are: MOLST covers a variety of end-of-life treatments. A DNR only gives instructions about CPR. The MOLST form can also be used in a community setting where the DNR is intended to be used as a directive in a hospital setting.
Our user reviews speak for themselves
Read more or give pdfFiller a try to experience the benefits for yourself
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
Can I create an electronic signature for signing my NY DOH-5003 in Gmail?
When you use pdfFiller's add-on for Gmail, you can add or type a signature. You can also draw a signature. pdfFiller lets you eSign your NY DOH-5003 and other documents right from your email. In order to keep signed documents and your own signatures, you need to sign up for an account.
How do I edit NY DOH-5003 straight from my smartphone?
The pdfFiller apps for iOS and Android smartphones are available in the Apple Store and Google Play Store. You may also get the program at https://edit-pdf-ios-android.pdffiller.com/. Open the web app, sign in, and start editing NY DOH-5003.
How do I edit NY DOH-5003 on an Android device?
You can edit, sign, and distribute NY DOH-5003 on your mobile device from anywhere using the pdfFiller mobile app for Android; all you need is an internet connection. Download the app and begin streamlining your document workflow from anywhere.
What is NY DOH-5003?
NY DOH-5003 is a form used for reporting certain health-related data to the New York State Department of Health.
Who is required to file NY DOH-5003?
Healthcare providers and facilities that are mandated by state law to report specific health information are required to file NY DOH-5003.
How to fill out NY DOH-5003?
To fill out NY DOH-5003, complete the sections with accurate data as required, ensuring all fields are filled out according to the guidelines provided by the New York State Department of Health.
What is the purpose of NY DOH-5003?
The purpose of NY DOH-5003 is to collect data that helps monitor public health, track disease trends, and ensure compliance with state health regulations.
What information must be reported on NY DOH-5003?
Information required on NY DOH-5003 typically includes patient demographics, health conditions treated, treatment dates, and other pertinent health-related data as specified by the reporting guidelines.
Fill out your NY DOH-5003 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
NY DOH-5003 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
