
Get the free Medication Administration Form Sample 2003-2004.doc - images pcmac
Show details
SLOW COUNTY SCHOOLS STUDENT HEALTH SERVICES Permission for Prescribed Medication to Be Given During School Hours TO BE COMPLETED BY PARENT/GUARDIAN: Date: School: Teacher/Grade: Name of Student: Date
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign medication administration form sample
Edit your medication administration form sample form online
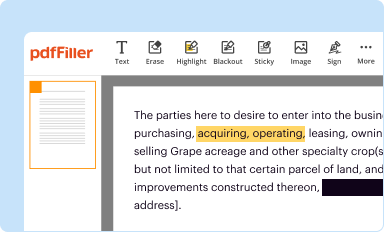
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
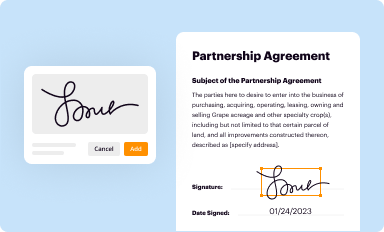
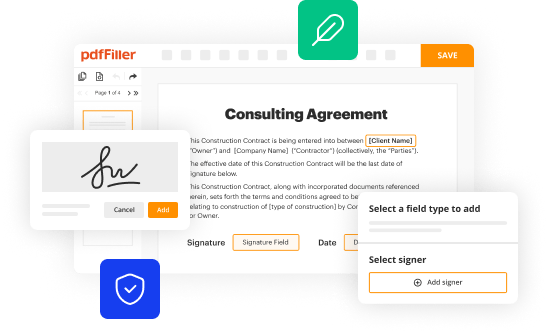
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
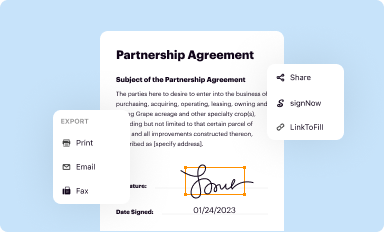
Share your form instantly
Email, fax, or share your medication administration form sample form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit medication administration form sample online



To use the services of a skilled PDF editor, follow these steps:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Upload a file. Select Add New on your Dashboard and upload a file from your device or import it from the cloud, online, or internal mail. Then click Edit.
3
Edit medication administration form sample. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
With pdfFiller, it's always easy to work with documents.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out medication administration form sample
To fill out a medication administration form sample, follow these steps:
01
Start by carefully reading the form and familiarizing yourself with the required information.
02
Begin filling out the form by providing the patient's personal details, such as their name, date of birth, and medical record number.
03
Next, enter the date and time of administering the medication, as well as the name and dosage of the medication being administered.
04
Include any specific instructions or directions provided by the prescribing healthcare professional.
05
If applicable, document the route of administration, such as oral, intravenous, or topical.
06
Indicate the reason for administering the medication, whether it is for pain management, infection control, or other therapeutic purposes.
07
Note any adverse reactions or side effects experienced by the patient during or after medication administration.
08
Finally, ensure that the form is signed and dated by the individual administering the medication.
8.1
Medication administration form samples are crucial for various healthcare professionals and institutions, including:
09
Nurses: Registered nurses and nursing staff in hospitals, clinics, and long-term care facilities use medication administration forms to record the details of medications given to patients.
10
Caregivers: Home healthcare providers and family caregivers who assist individuals with their medication management rely on these forms to maintain accurate records.
11
Pharmacists: Pharmacists may use medication administration forms to document medication counseling provided to patients and track their adherence to prescribed medications.
12
Medical facilities: Hospitals, clinics, and healthcare facilities often require medication administration forms to comply with legal, regulatory, and billing requirements.
Remember, medication administration forms are essential tools for ensuring patient safety, facilitating effective communication within healthcare teams, and maintaining accurate records of medication administration.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I send medication administration form sample for eSignature?
When you're ready to share your medication administration form sample, you can swiftly email it to others and receive the eSigned document back. You may send your PDF through email, fax, text message, or USPS mail, or you can notarize it online. All of this may be done without ever leaving your account.
How do I edit medication administration form sample online?
pdfFiller not only allows you to edit the content of your files but fully rearrange them by changing the number and sequence of pages. Upload your medication administration form sample to the editor and make any required adjustments in a couple of clicks. The editor enables you to blackout, type, and erase text in PDFs, add images, sticky notes and text boxes, and much more.
Can I create an electronic signature for the medication administration form sample in Chrome?
As a PDF editor and form builder, pdfFiller has a lot of features. It also has a powerful e-signature tool that you can add to your Chrome browser. With our extension, you can type, draw, or take a picture of your signature with your webcam to make your legally-binding eSignature. Choose how you want to sign your medication administration form sample and you'll be done in minutes.
What is medication administration form sample?
The medication administration form sample is a document used to record the administration of medication to a patient.
Who is required to file medication administration form sample?
Healthcare providers or caregivers who administer medication to patients are required to file the medication administration form sample.
How to fill out medication administration form sample?
The medication administration form sample should be filled out by documenting the medication given, dosage, time administered, route of administration, and any other relevant information.
What is the purpose of medication administration form sample?
The purpose of the medication administration form sample is to ensure accurate and timely recording of medication administration to monitor patient's health and responses to medication.
What information must be reported on medication administration form sample?
Information that must be reported on the medication administration form sample includes patient's name, date and time of administration, medication name, dosage, route of administration, and any observations or reactions.
Fill out your medication administration form sample online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Medication Administration Form Sample is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
