VA-003A-WC free printable template
Show details
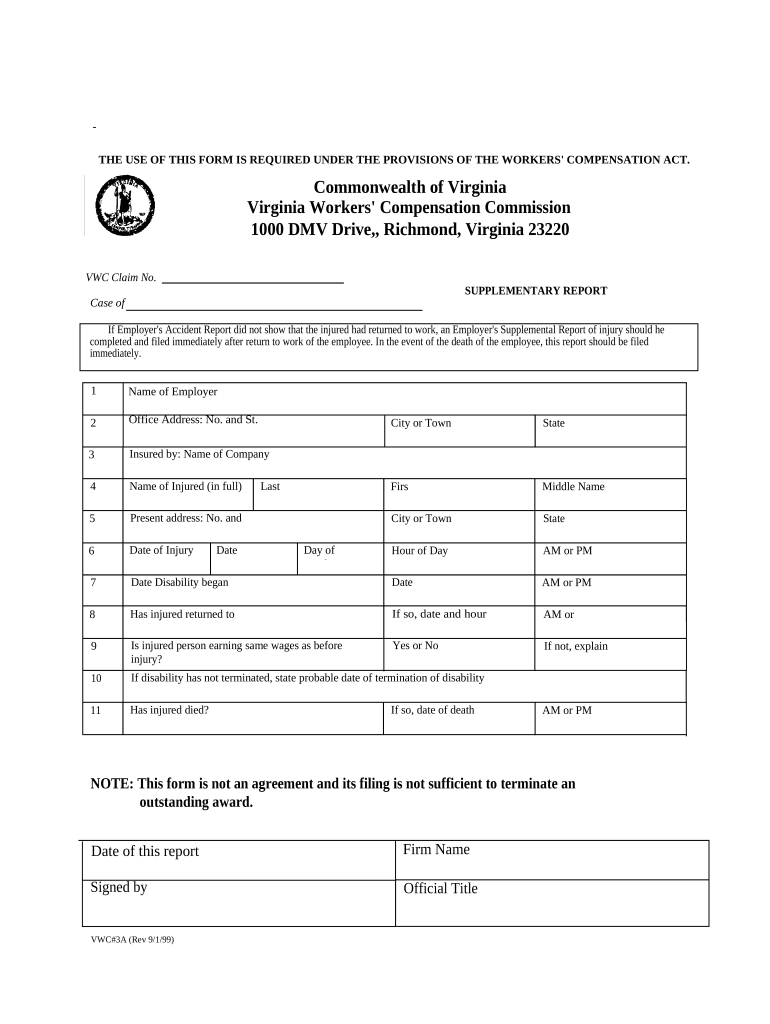
THE USE OF THIS FORM IS REQUIRED UNDER THE PROVISIONS OF THE WORKERS' COMPENSATION ACT.
Commonwealth of Virginia
Virginia Workers' Compensation Commission
1000 DMV Drive,, Richmond, Virginia 23220
VWC Claim No.
SUPPLEMENTARY REPORT
Case of
If Employer's Accident Report did not show that the injured had returned to work, an Employer's Supplemental Report of injury should he
completed and filed immediately after return to work of the employee. In the event of the death of the employee, this...report should be filed
immediately.
1
Name of Employer
2
Office Address: No. and St.
3
Insured by: Name of Company
4
Name of Injured (in full)
5
Present address: No. and
St.
6
Date of Injury
7
City or Town
State
Firs
t
Middle Name
City or Town
State
Hour of Day
AM or PM
Date Disability began
Date
AM or PM
8
Has injured returned to
work?
If so, date and hour
AM or
PM
9
Is injured person earning same wages as before
injury?
Yes or No
If not, explain
10
If...disability has not terminated, state probable date of termination of disability
11
Has injured died?
Date
Last
Day of
Week
If so, date of death
AM or PM
NOTE: This form is not an agreement and its filing is not sufficient to terminate an
outstanding award.
Date of this report
Firm Name
Signed by
Official Title
VWC#3A (Rev 9/1/99)
pdfFiller is not affiliated with any government organization
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why choose pdfFiller for your legal forms?
All-in-one solution
pdfFiller offers a PDF editor, eSignatures, file sharing, collaboration tools, and secure storage—all in one place.
Easy to use
pdfFiller is simple, cloud-based, has a mobile app, and requires no downloads or a steep learning curve.
Secure and compliant
With encryption, user authentication, and certifications like HIPAA, SOC 2 Type II, and PCI DSS, pdfFiller keeps sensitive legal forms secure.
What is VA-003A-WC
VA-003A-WC is a form used for filing a workers' compensation claim within the Virginia Department of Veterans Affairs.
pdfFiller scores top ratings on review platforms
It's a great program, but it can be a bit glitch-y when trying to fill in information. A minor problem, but it does get in the way of having an optimal user experience
excellent program! So easy to use. I recommend to everyone.
Excellent product from an incredible organization.
A little tough to regenerate the template. Not that user-friendly
It would be a 5 if I could open multiple docs for editing and switch from one to the other rather than closing one to open another.
Where to find spell check. Difficulty inserting or changing words.
Who needs VA-003A-WC?
Explore how professionals across industries use pdfFiller.

VA-003A-WC is needed by:
-
Veterans seeking workers' compensation.
-
Employers processing a claim for a veteran employee.
-
Legal representatives assisting veterans with claims.
-
Veterans service organizations supporting claim submissions.
How to fill out the VA-003A-WC
-
1.Open the VA-003A-WC form using pdfFiller.
-
2.Begin by entering the veteran's full name in the designated field.
-
3.Provide the veteran's social security number to identify the claimant.
-
4.Fill in the date of the injury, ensuring it matches any supporting documentation.
-
5.Complete the section describing the nature of the injury – be detailed and precise.
-
6.Enter the veteran's contact information, including a phone number and email address.
-
7.If applicable, list any witnesses to the incident by providing their names and contact information.
-
8.Check the box that corresponds to the type of benefits being requested.
-
9.Review the form for accuracy and completeness before submitting.
-
10.Use the 'Save' function to keep a copy for personal records and then submit the form as instructed.
Related Forms
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.