Last updated on May 20, 2026
Get the free Physician Orders for Life-Sustaining Treatment (POLST)
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is physician orders for life-sustaining
The Physician Orders for Life-Sustaining Treatment (POLST) is a medical document used by patients and healthcare professionals to outline a patient's preferences for life-sustaining treatments based on their medical condition.
pdfFiller scores top ratings on review platforms
Who needs physician orders for life-sustaining?
Explore how professionals across industries use pdfFiller.

Physician orders for life-sustaining is needed by:
-
Patients with serious illnesses wanting to specify treatment preferences
-
Legal surrogates making healthcare decisions on behalf of a patient
-
Physicians, ARNPs, and PAs providing medical care
-
Healthcare facilities managing patient transfer or discharge
-
Hospices and palliative care providers
-
Family members involved in advanced care planning
Comprehensive Guide to physician orders for life-sustaining
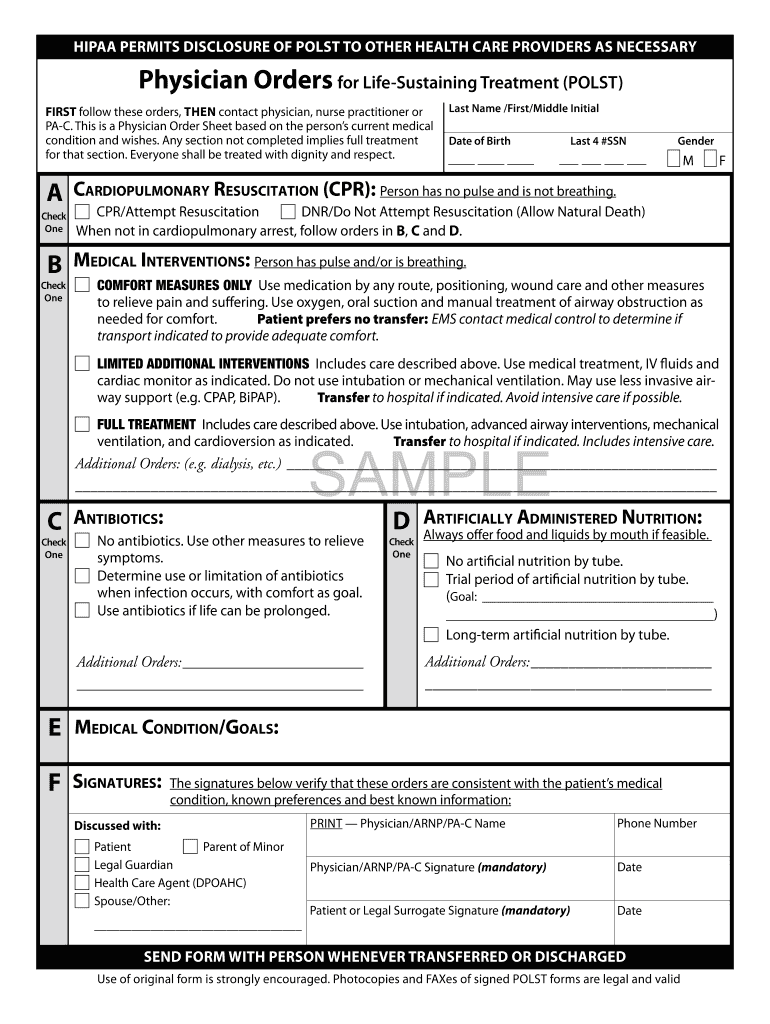
What is the Physician Orders for Life-Sustaining Treatment (POLST)?
The Physician Orders for Life-Sustaining Treatment (POLST) form is a medical document used to specify a patient's preferences for life-sustaining treatments. It serves the crucial purpose of aligning medical care with patient wishes, ensuring that individuals receive the type of care they desire in critical situations. The form includes sections for cardiopulmonary resuscitation (CPR) preferences and medical interventions, allowing patients to convey their specific medical treatment preferences. Utilizing a POLST form template can significantly streamline the decision-making process during emergencies.
Purpose and Benefits of the POLST Form
The POLST form is vital for effective advance care planning and end-of-life care decisions. One of the key benefits is that it helps avoid unnecessary medical interventions, thereby respecting patient wishes in critical situations. The clarity provided by the POLST form ensures that healthcare providers can follow precise healthcare directives without confusion. This is especially important in emergencies when timely communication between healthcare providers and families is essential.
Key Features of the POLST Form
The POLST form includes several critical sections that explain the patient's choices, such as CPR preferences, nutrition options, and medical interventions. It is important to note that the form must contain signatures from both a healthcare provider and the patient or legal surrogate to be valid. Regular review and updates of the POLST are crucial, as these actions ensure that the form accurately reflects current medical treatment preferences.
-
CPR preferences
-
Medical interventions section
-
Nutrition section
-
Requirement of signatures
-
Periodic reviews and updates
Who Needs the POLST Form and Eligibility Criteria
The POLST form is particularly beneficial for patients with serious illnesses or those nearing the end of life. Various roles, including physicians, ARNPs, and PAs, play a significant role in the completion of this document. Understanding the eligibility criteria for patients and legal representatives is essential to ensure that the form serves its intended purpose effectively. This includes identifying individuals who may require the POLST, such as those lacking the capacity to make healthcare decisions.
How to Fill Out the POLST Form Online (Step-by-Step)
Filling out the POLST form electronically can be done easily through pdfFiller. Here’s a step-by-step guide to assist you:
-
Access the POLST form on pdfFiller.
-
Complete essential fields, including CPR preferences.
-
Ensure to include the necessary signatures for validity.
-
Review all entries for accuracy before finalizing.
-
Save your completed form for your records.
Review and Validation Checklist for the POLST Form
To ensure your POLST form is completed correctly, follow this validation checklist:
-
Check for common errors in filling out the form.
-
Verify the roles of signatories, including the healthcare provider and legal surrogate.
-
Ensure all entries match the patient's wishes.
How to Sign the POLST Form: Digital vs. Wet Signatures
Understanding the signature requirements for the POLST form is crucial. Digital signatures can be convenient, but it is vital to recognize the differences compared to wet signatures. Security considerations are paramount when handling sensitive medical data, so ensure that electronic signatures are adequately protected. Both the patient and the healthcare provider must sign the form for it to be valid.
How to Download, Save, and Print the POLST Form
After completing the POLST form on pdfFiller, users can follow these steps to manage the document:
-
Download the completed form from the platform.
-
Save the document securely on your device.
-
Print the POLST form correctly for distribution to relevant healthcare providers.
Where to Submit the POLST Form and What Happens Next
Upon completion, the POLST form should be submitted to various locations, including your primary care physician or local hospital. Tracking submissions is essential to confirm receipt and ensure compliance with patient wishes. Additionally, keeping multiple copies of the POLST form is recommended to maintain access across different healthcare settings.
Ensuring Security and Compliance for the POLST Form
When handling the POLST form, ensuring security and compliance is critical. pdfFiller employs 256-bit encryption and adheres to HIPAA and GDPR guidelines to protect sensitive information. To maintain the integrity of the POLST form, best practices for secure handling must be observed.
Empowering Your Healthcare Decisions with pdfFiller
pdfFiller provides an efficient means to complete the POLST form securely and conveniently. Users can take advantage of the platform’s capabilities to fill out forms, manage documents, and maintain secure access to healthcare directives. Start your form-filling journey with pdfFiller today to empower your healthcare decisions effectively.
How to fill out the physician orders for life-sustaining
-
1.To access the Physician Orders for Life-Sustaining Treatment (POLST) form on pdfFiller, visit the pdfFiller website and search for 'POLST form'. You may also directly upload the document if you have a saved copy.
-
2.Once the form is open, familiarize yourself with pdfFiller's interface, which includes various tools for editing fields. You can click on the fields to start entering information.
-
3.Before you begin filling out the form, gather all necessary details such as patient information, healthcare provider details, and specifics of treatment preferences, including resuscitation wishes and medical interventions.
-
4.As you proceed, ensure to fill in each section carefully. Use the checkboxes to denote preferences, and provide any additional information in the text fields. Pay attention to instructions on sections needing signatures.
-
5.After completing all fields, take a moment to review the form. Ensure that each choice accurately reflects the patient’s wishes. Check that all necessary signatures are accounted for.
-
6.Once satisfied with the content, you can save your work by clicking 'Save'. You can also download the completed document or choose to submit it directly through pdfFiller as per your requirements.

Who is eligible to complete the POLST form?
The POLST form can be completed by patients with serious illnesses who wish to specify their treatment preferences, as well as their legal surrogates. Healthcare professionals like physicians, ARNPs, and PAs are also authorized to assist.
What information is required to fill out the POLST form?
To fill out the POLST form, you need details about the patient's medical condition, treatment preferences regarding CPR, medical interventions, and nutrition, as well as relevant information about the patient and the signing healthcare provider.
How do I submit the POLST form after completion?
After completing the POLST form on pdfFiller, you can submit it either by printing and physically handing it to the relevant healthcare provider, or electronically by using the submit functionality in pdfFiller if applicable.
Are there any common mistakes to avoid when filling out the POLST form?
Common mistakes include leaving sections incomplete, not obtaining required signatures, and failing to regularly review the document to ensure it reflects current wishes. Always double-check for accuracy.
How often should the POLST form be reviewed?
It is recommended that the POLST form be reviewed periodically or whenever a patient’s health status changes. This ensures that the treatment preferences remain aligned with current wishes and medical conditions.
Is there a fee associated with using pdfFiller to complete the POLST form?
pdfFiller may impose fees for premium services, including form completion and submission. Check their pricing page for specific details on fees and subscriptions.
Can the POLST form be modified after it is signed?
Once the POLST form is signed by both the patient and healthcare provider, any modifications should be done with care. It is often advisable to complete a new form and ensure all parties involved are updated.
Related Forms




Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.