
BCBS CUT7087-1E 2018-2025 free printable template
Show details
Care first.+. Provider Inquiry Resolution Formally of health care plansINSTRUCTIONS
FOR PROVIDER USE Unimportant: Do not use this form for Appeals or corrected claims.
This form is to be used for
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign bcbs provider inquiry form
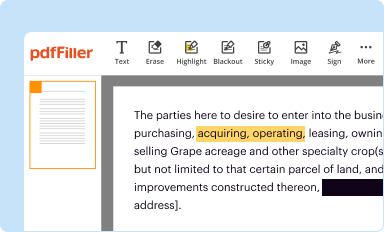
Edit your provider inquiry resolution form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
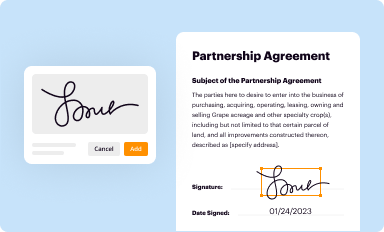
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
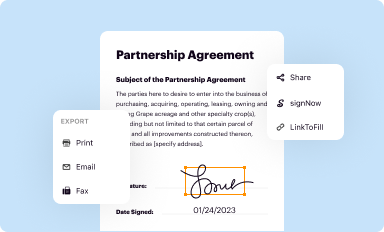
Share your form instantly
Email, fax, or share your information form provider form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit provider resolution online



In order to make advantage of the professional PDF editor, follow these steps below:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit provider inquiry create form. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
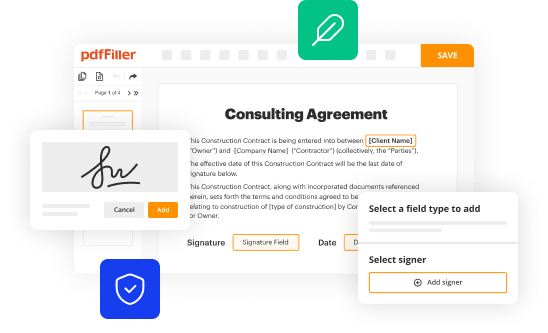
With pdfFiller, it's always easy to work with documents.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
BCBS CUT7087-1E Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out provider inquiry form
How to fill out BCBS CUT7087-1E
01
Start by downloading the BCBS CUT7087-1E form from the official Blue Cross Blue Shield website.
02
Carefully read the instructions provided with the form to understand the required information.
03
Fill in the patient’s demographic details such as name, address, and date of birth in the designated fields.
04
Provide the insurance policy number and group number as specified.
05
Accurately enter the details of the service being billed, including the date of service and procedure codes.
06
Include the provider's information, such as name, NPI number, and contact information.
07
Review the completed form for accuracy and ensure all required fields are filled out.
08
Submit the form according to your provider's submission guidelines, either electronically or via mail.
Who needs BCBS CUT7087-1E?
01
Patients who are receiving services covered by Blue Cross Blue Shield insurance.
02
Healthcare providers who are billing Blue Cross Blue Shield for services rendered.
03
Facilities that require reimbursement for medical services provided under BCBS coverage.
Fill
provider inquiry print
: Try Risk Free
People Also Ask about provider inquiry blank
What is the phone number for CareFirst md provider?
Comments or Questions for Us? If you have comments or questions, we want to help you. For technical support, call the CareFirst Help Desk at (877) 526 – 8390.
What is the prefix XXP Alpha for BCBS?
What BCBS plan starts with Xxp? By now, you should have received your new BCBS member ID card(s) your subscriber ID beginning with the 3-letter prefix 'XXP' indicating the PPO Deductible Plan. Please remember to update your medical providers and pharmacy with your new insurance information to avoid any claims issues.
What is CareFirst payer ID for medical claims?
Electronically (preferred method) through our Clearinghouse, Change Healthcare (formerly Emdeon) – Payor ID 45281.
What is the alpha prefix for CareFirst BCBS?
Member ID cards may include one of several logos identifying the type of coverage the member has and/or indicating the provider's reimbursement level. Unique prefix. CareFirst IDs have plan codes 080/580 and 190/690.
What is the group name for CareFirst?
CareFirst BlueCross BlueShield Medicare Advantage is the shared business name of CareFirst Advantage, Inc., CareFirst Advantage PPO, Inc.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I modify my bcbs resolution sample in Gmail?
pdfFiller’s add-on for Gmail enables you to create, edit, fill out and eSign your provider inquiry sample and any other documents you receive right in your inbox. Visit Google Workspace Marketplace and install pdfFiller for Gmail. Get rid of time-consuming steps and manage your documents and eSignatures effortlessly.
How can I get provider resolution pdf?
With pdfFiller, an all-in-one online tool for professional document management, it's easy to fill out documents. Over 25 million fillable forms are available on our website, and you can find the bcbs form cut7087 in a matter of seconds. Open it right away and start making it your own with help from advanced editing tools.
How do I edit bcbs inquiry blank straight from my smartphone?
The pdfFiller mobile applications for iOS and Android are the easiest way to edit documents on the go. You may get them from the Apple Store and Google Play. More info about the applications here. Install and log in to edit bcbs cut7087 make.
What is BCBS CUT7087-1E?
BCBS CUT7087-1E is a standard form used for reporting specific data related to Blue Cross Blue Shield programs.
Who is required to file BCBS CUT7087-1E?
Providers and organizations that participate in Blue Cross Blue Shield programs and need to report certain claims information are required to file BCBS CUT7087-1E.
How to fill out BCBS CUT7087-1E?
To fill out BCBS CUT7087-1E, you must provide accurate information regarding patient claims, provider details, and any applicable codes as outlined in the filing instructions.
What is the purpose of BCBS CUT7087-1E?
The purpose of BCBS CUT7087-1E is to ensure that accurate and consistent data is submitted for the processing of claims within Blue Cross Blue Shield programs.
What information must be reported on BCBS CUT7087-1E?
Information that must be reported includes patient demographics, service details, diagnosis codes, and provider information as specified in the form guidelines.
Fill out your provider resolution template 2018-2025 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Bcbs cut7087 Get is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
