Last updated on Apr 10, 2026
Get the free Medical History Questionnaire
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is medical history questionnaire
The Medical History Questionnaire is a healthcare form used by patients and physicians to collect essential medical history information for effective treatment.
pdfFiller scores top ratings on review platforms
Who needs medical history questionnaire?
Explore how professionals across industries use pdfFiller.

Medical history questionnaire is needed by:
-
Patients seeking medical care
-
Physicians requiring patient medical history
-
Healthcare providers for patient intake
-
Clinics and hospitals for efficient registration
-
Researchers studying patient health trends
Comprehensive Guide to medical history questionnaire
What is the Medical History Questionnaire?
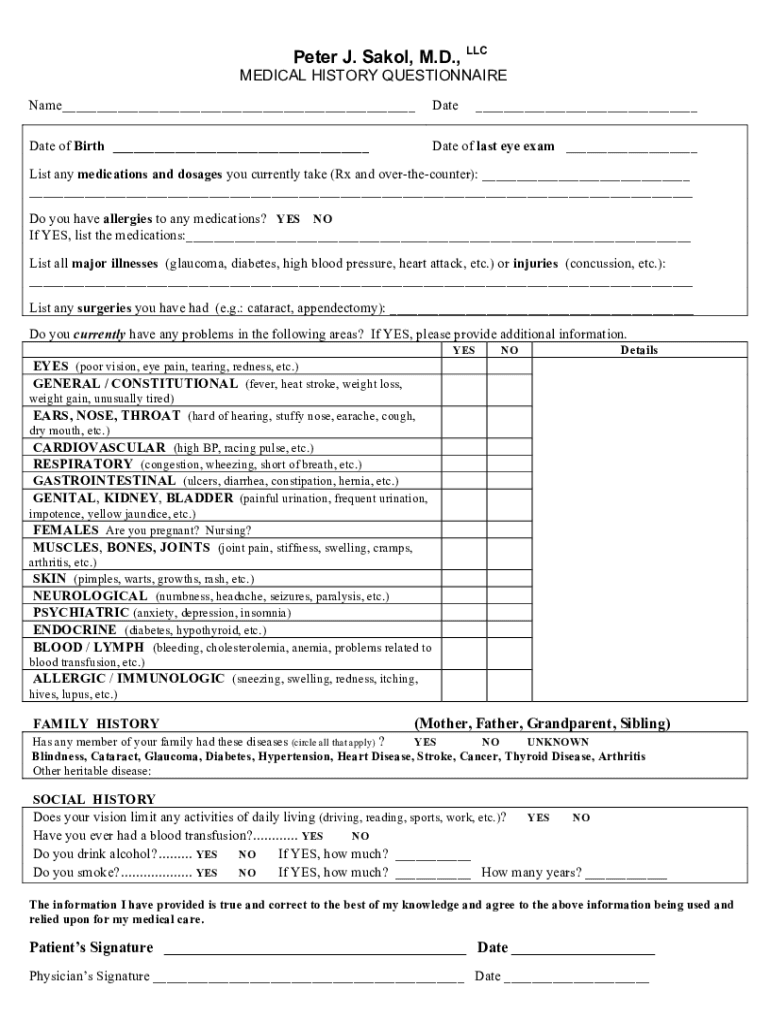
The Medical History Questionnaire is a vital tool for healthcare providers, designed to gather comprehensive medical history information from patients. This healthcare questionnaire plays a significant role in documenting essential details such as personal information, current medications, allergies, and past medical events. Accurate completion of the medical history form is critical as it ensures that healthcare professionals have the necessary information to provide effective care.
Purpose and Benefits of the Medical History Questionnaire
Completing the Medical History Questionnaire is crucial for a variety of reasons. It aids in accurate diagnosis and treatment planning, significantly enhancing patient outcomes. Moreover, both patients and physicians benefit from this process, as it streamlines communication and ensures that healthcare decisions are based on complete and accurate patient medical history. The healthcare intake form thus serves as a foundational element in the patient-physician relationship.
Key Features of the Medical History Questionnaire
The Medical History Questionnaire contains several key components essential for thorough patient assessment. Typical sections include:
-
Personal information
-
Current medications
-
Allergies
-
Major illnesses
-
Past surgeries
-
Family medical history
-
Social history
This medical questionnaire template is structured with fillable fields, checkboxes, and specified signature requirements to ensure clarity and completeness.
Who Needs the Medical History Questionnaire?
Various groups of individuals are required to complete the Medical History Questionnaire. It is essential for new patients seeking care, those experiencing changes in health status, and individuals preparing for medical procedures. This patient medical questionnaire supports physicians in delivering high-quality care by providing a comprehensive overview of each patient's health journey.
How to Fill Out the Medical History Questionnaire Online (Step-by-Step)
Completing the Medical History Questionnaire online using pdfFiller is straightforward. Follow these steps for an efficient process:
-
Access the medical history questionnaire template on pdfFiller.
-
Enter your personal information in the designated fields.
-
Provide details regarding current medications and allergies.
-
Review all sections for completeness before finalizing.
-
Sign the questionnaire digitally or in print format.
Gather all necessary information before starting to make the process smoother and more efficient.
Common Errors and How to Avoid Them
While filling out the Medical History Questionnaire, there are frequent mistakes that can compromise the quality of information provided. Common errors include incomplete sections or misinformation. To avoid pitfalls, consider the following checklist:
-
Verify the accuracy of all entered information.
-
Ensure every section of the form is completed.
-
Check for proper signature placement.
Signing the Medical History Questionnaire
Signing the Medical History Questionnaire is a crucial step for both patients and physicians. You can use either a digital signature or a wet signature, each having different legal implications. It is essential to confirm the accuracy of the information provided through these signatures, as they signify agreement and authenticity.
Submission Methods and What Happens After You Submit
Once the Medical History Questionnaire is completed, it is important to know how to submit it. Options for electronic submission through pdfFiller include:
-
Emailing the completed form directly.
-
Saving the form in the cloud for secure access.
-
Sending via fax or print if necessary.
After submission, patients can expect confirmation of receipt along with assurances regarding the privacy of their sensitive information.
Security and Compliance for the Medical History Questionnaire
Concerns about data security and compliance are paramount when handling the Medical History Questionnaire. pdfFiller adheres to HIPAA and GDPR compliance regulations, ensuring that all medical forms are managed with the utmost care. The platform employs 256-bit encryption and follows SOC 2 Type II standards to protect sensitive medical information effectively.
Empower Your Healthcare Journey with pdfFiller
Utilizing pdfFiller to complete your Medical History Questionnaire offers numerous advantages. The platform provides a user-friendly interface with robust security features, enhancing the efficiency of filling out forms online. By streamlining the intake process, pdfFiller simplifies interactions between patients and healthcare providers, making healthcare management more effective.
How to fill out the medical history questionnaire
-
1.Access pdfFiller and search for 'Medical History Questionnaire' in the search bar.
-
2.Click on the document to open it in the editor.
-
3.Review the form sections which include personal information, current medications, allergies, surgeries, and family history.
-
4.Gather necessary information, such as your medications list and health conditions, to fill out the form accurately.
-
5.Use pdfFiller's tools to fill in the blank fields, check checkboxes, and enter your responses clearly.
-
6.Sign the form in the designated area for the patient and ensure your physician does the same.
-
7.After completing, review all entries for accuracy and clarity.
-
8.Use the toolbar to save your work or select the download option to keep a copy of the filled form.
-
9.Consider submitting the form directly via pdfFiller if your healthcare provider accepts online submissions.

Who needs to fill out the Medical History Questionnaire?
Both patients and physicians need to complete the Medical History Questionnaire. Patients provide their medical details while physicians verify and confirm the information is accurate.
Is there a time limit for completing the Medical History Questionnaire?
No specific deadline is generally set for completing the Medical History Questionnaire. However, it is advisable to fill it out before your scheduled medical appointment for an efficient consultation.
How should I submit the Medical History Questionnaire?
The form can be submitted physically at your healthcare provider's office or downloaded and emailed if allowed. Some providers may accept submissions through pdfFiller directly.
What information do I need to complete the Medical History Questionnaire?
You will need to provide personal information, current medications, any known allergies, major illnesses, surgeries, and family medical history. Have this information ready before starting the questionnaire.
What are common mistakes to avoid when filling this form?
Ensure you do not leave any required fields blank and double-check spellings, especially for medications and allergies. Also, avoid rushing through signature requirements to ensure accuracy.
How long does it take to process the Medical History Questionnaire?
Processing time for the Medical History Questionnaire may vary by provider, but expect feedback or further instructions within a few days after submission.
Can I get help if I find it challenging to fill out the form?
Yes, seeking assistance from your healthcare provider or family member is encouraged if you encounter challenges. They can help clarify questions or the information needed.
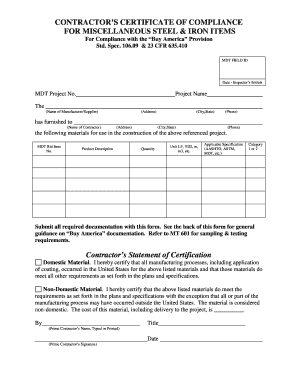
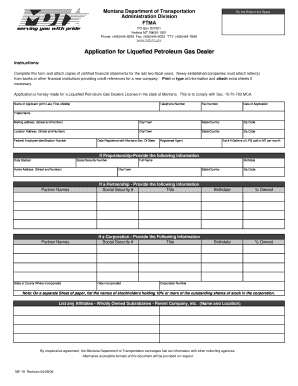
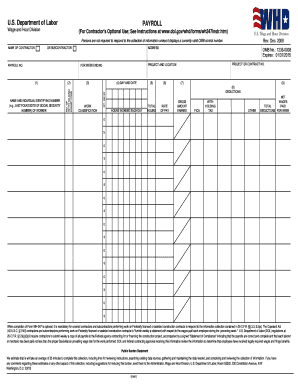
Related Forms


Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.