Get the free Request Your Medical Records - Cheyenne VA Medical Center
Show details
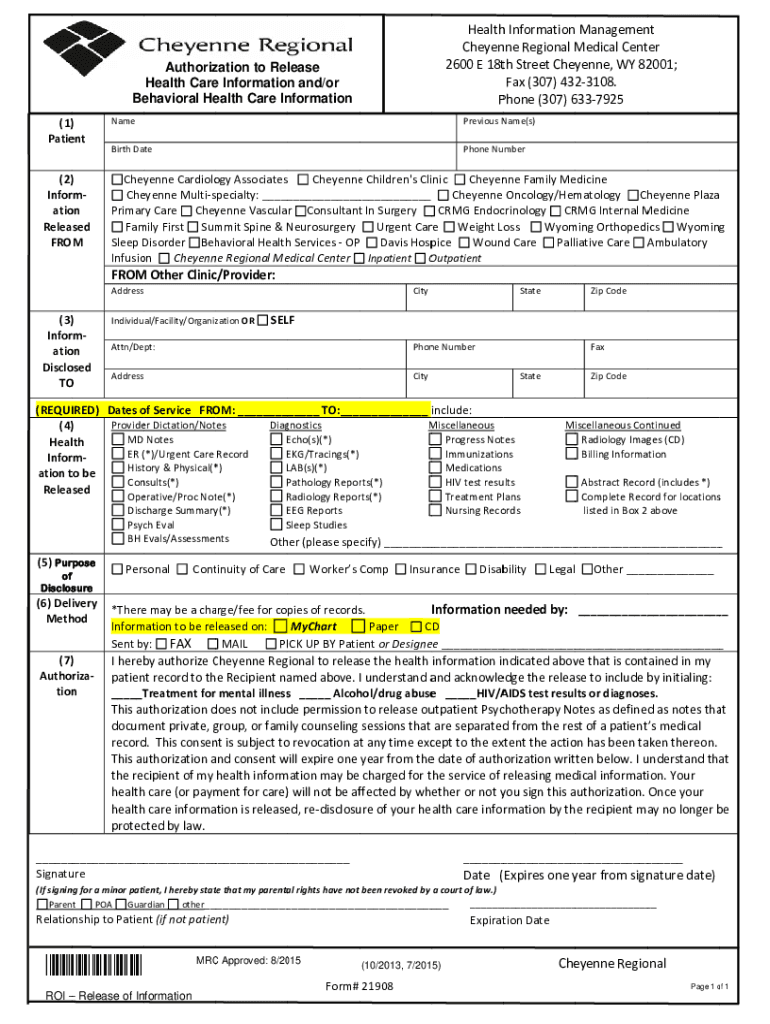
Health hInformationManagemen NT Chain nneRegionalM MedicalCentter 2600E18tthStreetCheyyenne,WY82 2001; Fax(307)432 23108. Phone(307)6 6337925Authoriz nation to Release Health Care e Information and/or
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign request your medical records
Edit your request your medical records form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your request your medical records form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing request your medical records online



To use the services of a skilled PDF editor, follow these steps below:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit request your medical records. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
With pdfFiller, dealing with documents is always straightforward.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out request your medical records
How to fill out request your medical records
01
Start by obtaining a copy of the medical records request form from your healthcare provider or their website.
02
Carefully read all the instructions provided on the form to ensure you understand the process and requirements.
03
Fill in your personal information accurately, including your full name, date of birth, address, and contact details.
04
Specify the medical records you are requesting by providing relevant details such as the dates of treatment, specific healthcare provider(s), and types of records needed (e.g., lab results, diagnoses, medication history, etc.).
05
If there is a specific reason or purpose for requesting the records, make sure to include it in the appropriate section of the form.
06
Determine the method of delivery you prefer for receiving the records, such as by mail, email, or pick-up.
07
Check if there are any fees associated with obtaining the medical records and arrange for payment if required (include this information on the form).
08
Review the completed form for accuracy and ensure all required fields are filled in.
09
Sign and date the request form, acknowledging that you understand the terms and conditions.
10
Make a copy of the completed form for your records, if needed, and submit the original form to your healthcare provider via the designated method (mail, fax, drop-off, etc.).
11
Keep a record of the date the request was submitted and any confirmation or reference numbers provided by the healthcare provider.
12
Allow a reasonable amount of time for the healthcare provider to process your request and deliver the medical records to you.
Who needs request your medical records?
01
Various individuals may need to request their medical records for different reasons, including:
02
- Patients who want to review their own medical history or share it with another healthcare provider.
03
- Individuals applying for disability benefits or insurance claims, as medical records may be required as supporting documentation.
04
- Researchers conducting medical studies or clinical trials, who may need access to specific medical records for analysis and evaluation.
05
- Legal professionals involved in medical malpractice or personal injury cases, who may need medical records as evidence or for expert opinions.
06
- Family members or caregivers who have legal authority or permission to manage the medical affairs of someone unable to do so themselves.
07
- Employers requesting medical records as part of employment-related background checks or health assessments.
08
- Educational institutions requiring medical records during the enrollment process, particularly for healthcare-related programs.
09
It is important to note that the specific requirements, procedures, and regulations for requesting medical records may vary depending on the country, healthcare provider, and purpose of the request. It is advisable to consult the applicable guidelines or seek assistance from the healthcare provider if needed.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I manage my request your medical records directly from Gmail?
You may use pdfFiller's Gmail add-on to change, fill out, and eSign your request your medical records as well as other documents directly in your inbox by using the pdfFiller add-on for Gmail. pdfFiller for Gmail may be found on the Google Workspace Marketplace. Use the time you would have spent dealing with your papers and eSignatures for more vital tasks instead.
How can I send request your medical records to be eSigned by others?
request your medical records is ready when you're ready to send it out. With pdfFiller, you can send it out securely and get signatures in just a few clicks. PDFs can be sent to you by email, text message, fax, USPS mail, or notarized on your account. You can do this right from your account. Become a member right now and try it out for yourself!
How do I execute request your medical records online?
Easy online request your medical records completion using pdfFiller. Also, it allows you to legally eSign your form and change original PDF material. Create a free account and manage documents online.
What is request your medical records?
A request for medical records is a formal process by which a patient or their authorized representative asks for access to their medical history and associated health information maintained by healthcare providers.
Who is required to file request your medical records?
Patients, or their legal representatives such as parents or guardians for minors, are required to file a request to obtain their medical records.
How to fill out request your medical records?
To fill out a request for medical records, one typically needs to complete a designated form provided by the healthcare provider, including personal identification details, the specific information requested, and any required signatures.
What is the purpose of request your medical records?
The purpose of requesting medical records is to obtain accurate health information for personal review, to share with other healthcare providers, or for legal, insurance, or personal reasons.
What information must be reported on request your medical records?
The request must usually include the patient's full name, date of birth, contact information, specific records requested, and if necessary, the patient's signature authorizing the release of information.
Fill out your request your medical records online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Request Your Medical Records is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
