Get the free New Patient Referral Form - akdhc.com
Show details
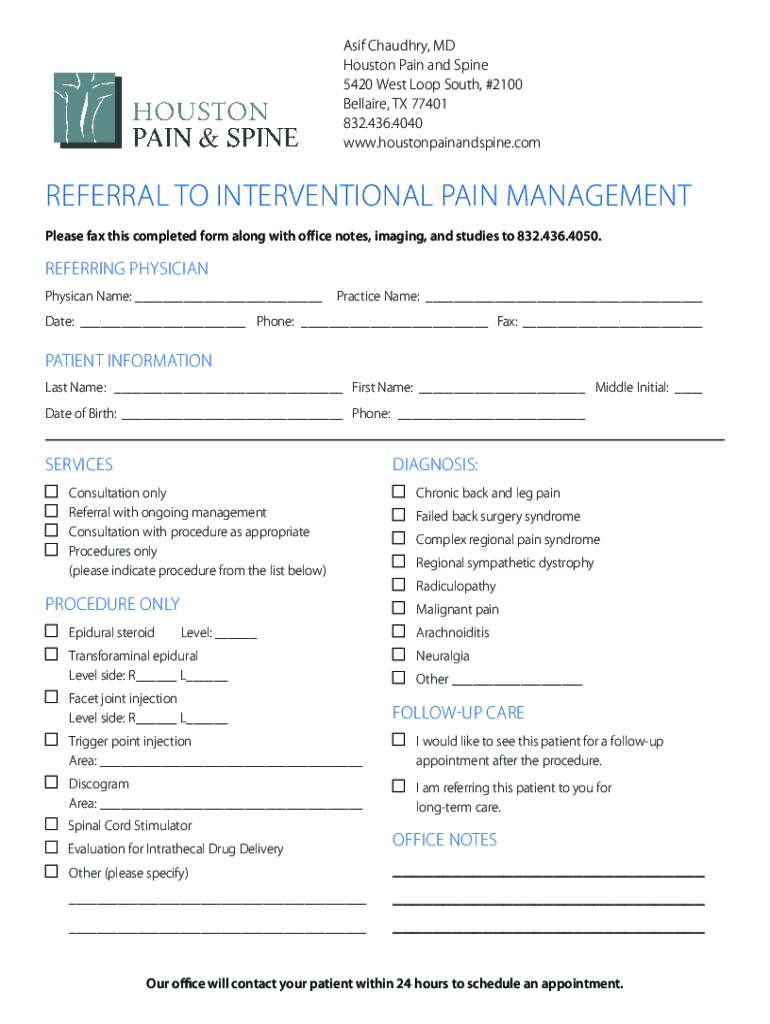
Asif Chaudhary, MD Houston Pain and Spine 5420 West Loop South, #2100 Bella ire, TX 77401 832.436.4040 www.houstonpainandspine.comRefeRRaL to inteRventionaL Pain management Please fax this completed
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign new patient referral form
Edit your new patient referral form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your new patient referral form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing new patient referral form online



Follow the guidelines below to take advantage of the professional PDF editor:
1
Register the account. Begin by clicking Start Free Trial and create a profile if you are a new user.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit new patient referral form. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Save your file. Choose it from the list of records. Then, shift the pointer to the right toolbar and select one of the several exporting methods: save it in multiple formats, download it as a PDF, email it, or save it to the cloud.
With pdfFiller, it's always easy to work with documents.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out new patient referral form
How to fill out new patient referral form
01
Begin by obtaining the new patient referral form from the healthcare provider or medical facility.
02
Read the instructions provided on the form carefully to ensure accurate completion.
03
Fill in the patient's personal information, such as their full name, date of birth, address, and contact details.
04
Provide the referring healthcare provider's information, including their name, contact information, and specialty.
05
Indicate the reason for referral, specifying the medical condition or concern that requires attention.
06
If any medical tests or imaging studies are attached and relevant to the referral, make sure to include them.
07
Sign and date the form to authenticate the information provided.
08
Review the completed form for any errors or missing information before submitting it.
09
Submit the filled-out new patient referral form to the designated healthcare facility or healthcare provider through the designated channel, which could be in-person, via mail, fax, or electronic submission.
10
Follow up with the referring healthcare provider or medical facility to ensure that the referral has been received and processed.
Who needs new patient referral form?
01
Any individual who requires medical attention or specialized care from a healthcare provider outside of their usual network or primary care physician may need to fill out a new patient referral form. Patients who are seeking specialized consultation, diagnostic tests, procedures, or treatments typically require a referral. Additionally, individuals who have chosen a new primary care provider or have relocated and need to establish a new healthcare provider often need to complete a new patient referral form.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I manage my new patient referral form directly from Gmail?
It's easy to use pdfFiller's Gmail add-on to make and edit your new patient referral form and any other documents you get right in your email. You can also eSign them. Take a look at the Google Workspace Marketplace and get pdfFiller for Gmail. Get rid of the time-consuming steps and easily manage your documents and eSignatures with the help of an app.
How do I execute new patient referral form online?
pdfFiller makes it easy to finish and sign new patient referral form online. It lets you make changes to original PDF content, highlight, black out, erase, and write text anywhere on a page, legally eSign your form, and more, all from one place. Create a free account and use the web to keep track of professional documents.
How do I edit new patient referral form on an Android device?
Yes, you can. With the pdfFiller mobile app for Android, you can edit, sign, and share new patient referral form on your mobile device from any location; only an internet connection is needed. Get the app and start to streamline your document workflow from anywhere.
What is new patient referral form?
A new patient referral form is a document used by healthcare providers to refer patients to specialists or other healthcare facilities for further examination, treatment, or consultation.
Who is required to file new patient referral form?
Healthcare providers, such as primary care physicians, are typically required to file a new patient referral form when referring a patient to a specialist.
How to fill out new patient referral form?
To fill out a new patient referral form, you need to provide patient information, referring provider details, the reason for referral, and any relevant medical history or documents that may assist the specialist.
What is the purpose of new patient referral form?
The purpose of the new patient referral form is to ensure proper communication and transfer of patient information between healthcare providers, facilitating coordinated care.
What information must be reported on new patient referral form?
The referral form generally requires the patient's name, date of birth, contact information, insurance details, the referring provider's information, and specifics about the medical issue being referred.
Fill out your new patient referral form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
New Patient Referral Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
