Last updated on Apr 10, 2026
Get the free Pharmacy Prior Authorization Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is pharmacy prior authorization request
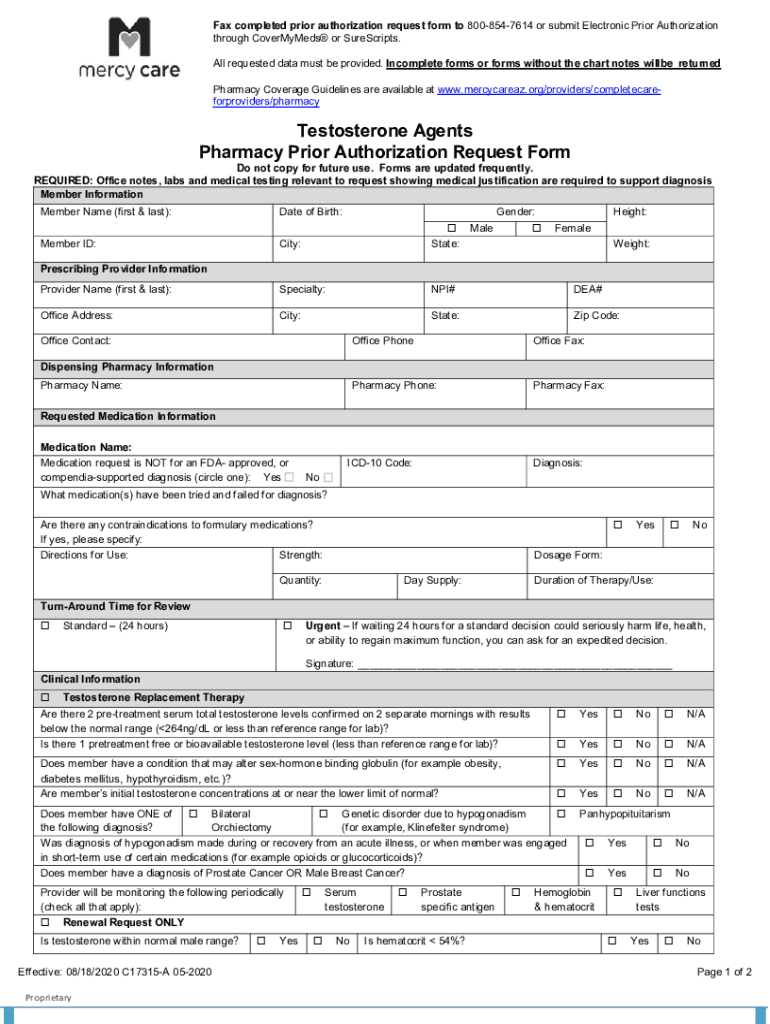
The Pharmacy Prior Authorization Request Form is a medical consent document used by healthcare providers in Arizona to request prior authorization for specific medications, particularly testosterone agents.
pdfFiller scores top ratings on review platforms
Who needs pharmacy prior authorization request?
Explore how professionals across industries use pdfFiller.

Pharmacy prior authorization request is needed by:
-
Healthcare providers prescribing testosterone agents
-
Pharmacists processing medication requests
-
Medical offices managing patient medications
-
Insurance professionals reviewing authorization requests
-
Patients seeking testosterone treatment
Comprehensive Guide to pharmacy prior authorization request
What is the Pharmacy Prior Authorization Request Form?
The Pharmacy Prior Authorization Request Form is a crucial document used by healthcare providers in Arizona to facilitate the approval process for specific medications, especially testosterone agents. This form enables prescribers to submit a request for prior authorization, ensuring that patients receive necessary treatments promptly. Understanding the significance of prior authorization helps in managing patient care and medication costs effectively.
Why Use the Pharmacy Prior Authorization Request Form?
Utilizing the Pharmacy Prior Authorization Request Form offers numerous benefits for healthcare providers and patients alike. This medical justification form streamlines the approval process, reducing delays in treatment. Moreover, it can lead to significant cost savings for patients and insurance providers, making it a vital tool in the healthcare system.
Key Features of the Pharmacy Prior Authorization Request Form
The Pharmacy Prior Authorization Request Form contains essential features to assist in the submission process. Required fields include:
-
Member information such as name and insurance details.
-
Provider details including contact information.
-
Medical justification and clinical data to support the request.
These components ensure that the healthcare provider form is complete and meets all necessary submission criteria.
Who Needs the Pharmacy Prior Authorization Request Form?
The primary audience for the Pharmacy Prior Authorization Request Form includes prescribing providers in Arizona who are responsible for submitting requests for their patients. Additionally, patients requiring testosterone treatment will benefit from understanding the necessity of this Arizona pharmacy form. Ensuring that all parties comprehend the process can enhance the efficacy of treatment approvals.
How to Fill Out the Pharmacy Prior Authorization Request Form Online
Filling out the Pharmacy Prior Authorization Request Form online using pdfFiller is straightforward. Follow these steps:
-
Access the form through the pdfFiller platform.
-
Enter the required information, including member name and prescribing provider details.
-
Utilize pdfFiller’s features to complete and eSign the form.
These steps provide a user-friendly approach to managing the prior authorization template efficiently.
Submission Process for the Pharmacy Prior Authorization Request Form
Once completed, the Pharmacy Prior Authorization Request Form can be submitted through several methods. Options include:
-
Online submission through the pdfFiller platform.
-
Faxing directly to the relevant pharmacy or insurance provider.
-
Mailing a hard copy to the intended recipient.
Be aware of turnaround times and potential delays in processing submissions to ensure timely medication access.
Common Errors and How to Avoid Them
During the form-filling process, there are common errors to watch out for. Frequent mistakes include:
-
Missing signatures on required fields.
-
Incomplete sections that provide necessary information.
To avoid these issues, validating the form before submission is critical. A thorough review and validation checklist can enhance the success rate of approval requests.
Security and Compliance When Using the Pharmacy Prior Authorization Request Form
Handling sensitive health information demands high levels of data security. pdfFiller employs robust security measures, including:
-
256-bit encryption to protect user data.
-
HIPAA compliance to safeguard patient privacy during the authorization process.
These security compliance features ensure that patient information remains confidential throughout the entire process.
How pdfFiller Can Help with Your Pharmacy Prior Authorization Request
pdfFiller enhances the experience of filling out the Pharmacy Prior Authorization Request Form with its comprehensive capabilities. Users can:
-
Edit text and images as necessary for personalization.
-
eSign the form directly within the platform.
-
Access and manage the form from any browser without the need for downloads.
This functionality through pdfFiller makes creating and submitting the pharmacy authorization template efficient and convenient.
Start Filling Out Your Pharmacy Prior Authorization Request Form Today!
Leverage the tools available through pdfFiller to simplify and secure your form-filling experience. Utilizing pdfFiller enhances the management of healthcare documentation, ensuring that you can focus on patient care without the added burden of paperwork.
How to fill out the pharmacy prior authorization request
-
1.To access the Pharmacy Prior Authorization Request Form, visit pdfFiller and log in to your account or create a new one if necessary.
-
2.Once logged in, use the search bar to locate the specific form by entering its name or related keywords.
-
3.Open the form and familiarize yourself with its layout. You will find sections for member information, provider details, and clinical data.
-
4.Before filling out the form, gather the necessary information. This includes the patient's name, prescription details, medical justification, and any relevant clinical data.
-
5.Begin by filling in the member name with the first and last name of the patient accurately.
-
6.Proceed to the provider details section, including your name, contact information, and any required identifiers.
-
7.Enter detailed medical justification for the requested medication, explaining the necessity and relevance of the treatment.
-
8.As you complete each field, ensure that all entries are clear and legible. Use pdfFiller's tools to check for errors or omissions.
-
9.Once all required fields are filled, carefully review the entire form. Verify accuracy in patient and provider information as well as medical justifications.
-
10.To finalize the form, sign the document where indicated. Use pdfFiller's signature tool to add your electronic signature if applicable.
-
11.After signing, save your work by clicking the save option. You can also download the completed form in your preferred format, typically PDF.
-
12.If submitting the form electronically, use the submit feature available on pdfFiller to send it directly to the appropriate insurance or pharmacy.

Who is eligible to use the Pharmacy Prior Authorization Request Form?
Healthcare providers in Arizona prescribing medications, especially testosterone agents, are eligible to use this form to request prior authorization from insurance companies.
Are there deadlines for submitting this form?
While specific deadlines may vary by insurer, it is best to submit the Pharmacy Prior Authorization Request Form as soon as possible after prescription issuance to avoid treatment delays.
How do I submit the completed form?
You can submit the completed Pharmacy Prior Authorization Request Form either electronically via pdfFiller or by printing it and sending it directly to the intended insurance provider or pharmacy.
What supporting documents should accompany the form?
With the Pharmacy Prior Authorization Request Form, you may need to attach relevant clinical information, previous treatment records, or any other documentation that supports the medical justification for the prescribed treatment.
What common mistakes should I avoid when filling out this form?
Common mistakes include omitting critical patient or provider information, failing to provide clear medical justification, and not signing the form where required. Always review your entries before submission.
What are the processing times for authorization after submission?
Processing times for prior authorization requests vary depending on the insurance provider. Typically, it can take anywhere from a few days to two weeks for a decision to be made.
What should I do if my authorization request is denied?
If your authorization request is denied, review the denial notice for reasons, and consider discussing with the insurer or your healthcare provider about appealing the decision or providing additional information.
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.