NY DOH-3867 2011 free printable template
Show details
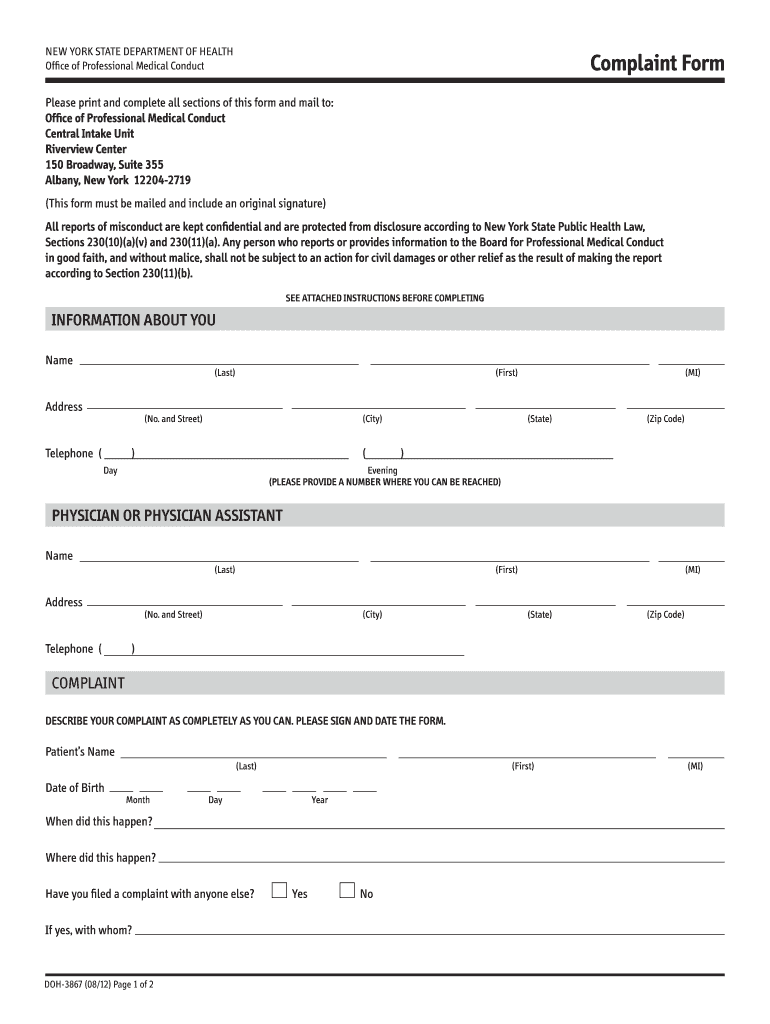
See attached Instructions before completing INFORMATION ABOUT YOU Name Address Last First No. and Street Telephone City Day MI State Zip Code Evening Please provide a number where you can be reached PHYSICIAN OR PHYSICIAN ASSISTANT COMPLAINT Describe your complaint as completely as you can. Please sign and date the form. Patient s Name Date of Birth Month Year When did this happen Have you filed a complaint with anyone else If yes with whom DOH-3...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign NY DOH-3867
Edit your NY DOH-3867 form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your NY DOH-3867 form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit NY DOH-3867 online



Follow the steps below to take advantage of the professional PDF editor:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit NY DOH-3867. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
With pdfFiller, it's always easy to work with documents.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
NY DOH-3867 Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out NY DOH-3867
How to fill out NY DOH-3867
01
Obtain the NY DOH-3867 form from the New York State Department of Health website or local office.
02
Fill in the applicant's name, address, and contact information in the designated sections.
03
Provide the details of the healthcare facility or provider in the appropriate fields.
04
Specify the type of health care services being requested.
05
Include any required documentation or supporting materials as stated in the form instructions.
06
Review the completed form for accuracy and completeness.
07
Sign and date the form as required.
08
Submit the filled-out form to the appropriate department via mail or online, if applicable.
Who needs NY DOH-3867?
01
Individuals seeking to authorize a healthcare provider to access their health records.
02
Patients who wish to grant permission for the release of their medical information.
03
Healthcare professionals needing to ensure compliance with health information privacy regulations.
04
Family members or legal guardians who need to manage the health information of a minor or incapacitated individual.
Fill
form
: Try Risk Free
People Also Ask about
How do I complain about a local pharmacy?
Each pharmacy must have a complaints manager. Their chief executive or a partner must act as the 'responsible person' who makes sure complaints are dealt with properly. You can complain by letter, email or by talking to someone at the pharmacy.
How do I file a complaint with NYS Dept of health?
Phone. 1-800-663-6114 - Complaints/Inquiries (Monday-Friday 9:00 a.m - 5:00 p.m.)
How do I report a doctor in NY?
Doctor Complaint Agency: New York State Department of Health. Division: Professional Medical Conduct. Phone Number: (800) 663-6114. Business Hours: Monday - Friday: 8 AM - 4:45 PM.
What is the example of complaint?
I wish to complain about _ (name of product or service, with serial number or account number) that I purchased on _ (date and location of transaction). I am complaining because _ (the reason you are dissatisfied). To resolve this problem I would like you to _ (what you want the business to do).
How do you make a proper complaint?
How to write an effective complaint letter Be clear and concise. State exactly what you want done and how long you're willing to wait for a response. Don't write an angry, sarcastic, or threatening letter. Include copies of relevant documents, like receipts, work orders, and warranties.
How do I fill out a complaint form?
0:31 2:02 Learn How to Fill the Complaint Form - YouTube YouTube Start of suggested clip End of suggested clip Next. You must provide your name as the plaintiff. And the names of any other individuals you may beMoreNext. You must provide your name as the plaintiff. And the names of any other individuals you may be representing as Co plaintiffs such as minor children or dependents.
How do I file a complaint with NYS Dept of Health?
Phone. 1-800-663-6114 - Complaints/Inquiries (Monday-Friday 9:00 a.m - 5:00 p.m.)
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I modify NY DOH-3867 without leaving Google Drive?
People who need to keep track of documents and fill out forms quickly can connect PDF Filler to their Google Docs account. This means that they can make, edit, and sign documents right from their Google Drive. Make your NY DOH-3867 into a fillable form that you can manage and sign from any internet-connected device with this add-on.
How do I edit NY DOH-3867 in Chrome?
NY DOH-3867 can be edited, filled out, and signed with the pdfFiller Google Chrome Extension. You can open the editor right from a Google search page with just one click. Fillable documents can be done on any web-connected device without leaving Chrome.
How do I complete NY DOH-3867 on an Android device?
Use the pdfFiller Android app to finish your NY DOH-3867 and other documents on your Android phone. The app has all the features you need to manage your documents, like editing content, eSigning, annotating, sharing files, and more. At any time, as long as there is an internet connection.
What is NY DOH-3867?
NY DOH-3867 is a form used to report and document certain health information as required by the New York State Department of Health.
Who is required to file NY DOH-3867?
Individuals or entities involved in specified health-related activities, such as healthcare providers or organizations, are typically required to file NY DOH-3867.
How to fill out NY DOH-3867?
To fill out NY DOH-3867, one must complete the required fields accurately, providing necessary documentation and following the instructions provided with the form.
What is the purpose of NY DOH-3867?
The purpose of NY DOH-3867 is to collect important health data for monitoring public health and ensuring compliance with state health regulations.
What information must be reported on NY DOH-3867?
The form requires reporting information such as specific health conditions, patient demographics, treatment details, and any other relevant health data mandated by the New York State Department of Health.
Fill out your NY DOH-3867 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
NY DOH-3867 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
