PA MR 543.02 2021 free printable template
Show details
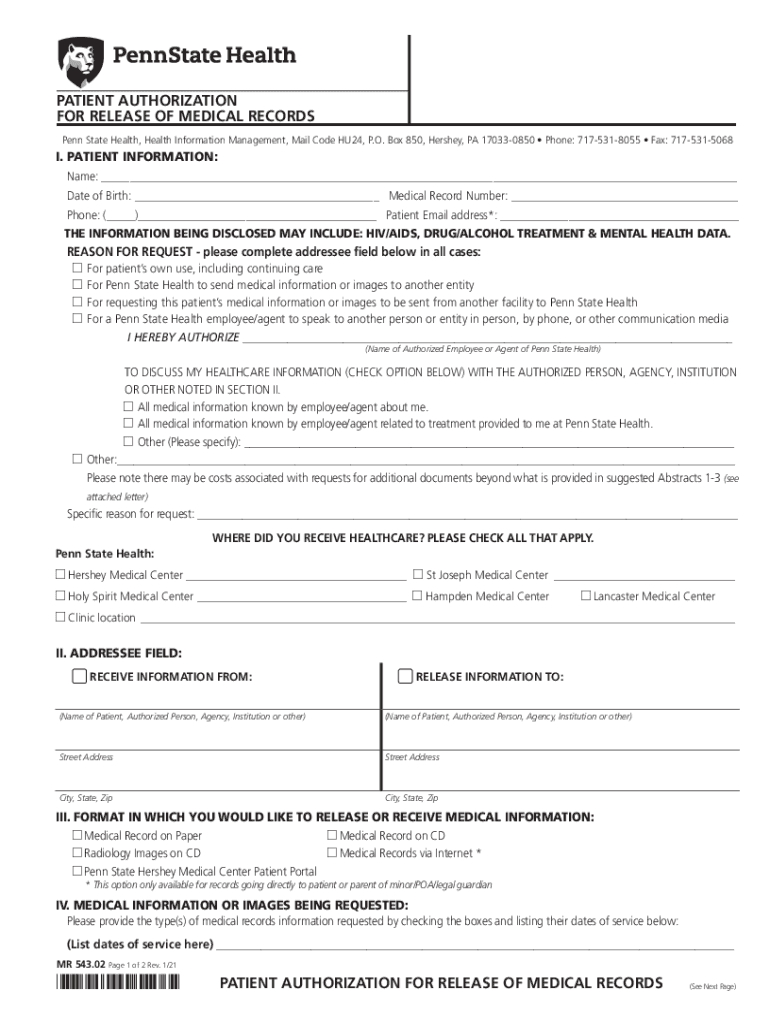
PATIENT AUTHORIZATION FOR RELEASE OF MEDICAL RECORDS Penn State Health, Health Information Management, Mail Code HU24, P.O. Box 850, Hershey, PA 170330850 Phone: 7175318055 Fax: 7175315068I. PATIENT
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign mr 54302 patient authorization

Edit your mr 54302 patient authorization form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your mr 54302 patient authorization form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit mr 54302 patient authorization online



Follow the guidelines below to take advantage of the professional PDF editor:
1
Log in to your account. Start Free Trial and register a profile if you don't have one.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit mr 54302 patient authorization. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Save your file. Select it in the list of your records. Then, move the cursor to the right toolbar and choose one of the available exporting methods: save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud.
It's easier to work with documents with pdfFiller than you could have believed. You can sign up for an account to see for yourself.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
PA MR 543.02 Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out mr 54302 patient authorization

How to fill out PA MR 543.02
01
Begin with personal information: Fill in your name, address, and contact details in the designated fields.
02
Specify the type of application: Clearly indicate whether it is for a new application, renewal, or modification.
03
Provide relevant dates: Enter the date of birth and any other critical dates requested.
04
Include financial information: Fill out any sections related to your income, expenses, and financial status accurately.
05
Complete all required signatures: Ensure that you and any other required signatories have signed the application.
06
Review all sections: Double-check that all information is accurate and complete before submission.
07
Submit the form: Send the completed PA MR 543.02 to the appropriate department, ensuring you keep a copy for your records.
Who needs PA MR 543.02?
01
Individuals seeking assistance with medical assistance programs in Pennsylvania.
02
Those applying for financial aid related to medical services.
03
Existing recipients who need to renew or modify their current assistance.
Fill
form
: Try Risk Free
People Also Ask about
What is an authorization to release health information?
An authorization is a detailed document that gives covered entities permission to use protected health information for specified purposes, which are generally other than treatment, payment, or health care operations, or to disclose protected health information to a third party specified by the individual.
How do I write a letter requesting medical information?
I was treated in your office [at your facility] between [fill in dates]. I request copies of the following [or all] health records related to my treatment. [Identify records requested (e.g., medical-history form you filled out; physician and nurses' notes; test results; consultations with specialists; referrals).]
What is included in the release of patient information?
The patient's legal name, date of birth, gender, Social Security number, address, telephone number, guarantor, subscriber, or next-of-kin are key identifying elements that assist in establishing the proper individual.
What is the process when releasing patient's medical records?
The physician should ask the patient to sign a written authorization to release this nontherapeutic information. The written permission should be dated, state to whom the information is to be released, which information may be passed on to that party, and when the permission to obtain information expires.
What is the purpose of a medical authorization?
Prior authorization (also called “preauthorization” and “precertification”) refers to a requirement by health plans for patients to obtain approval of a health care service or medication before the care is provided. This allows the plan to evaluate whether care is medically necessary and otherwise covered.
What form is used to allow the release of their medical records?
The medical record information release (HIPAA) form allows a patient to give authorization to a 3rd party and access their health records. The release also allows the added option for healthcare providers to share information.
Who authorizes release of medical information is the?
At the first patient encounter, the physician should have the patient sign an authorization to release information as necessary for the patient's treatment. This includes release to consulting physicians, laboratories, and other health care providers.
What does ROI stand for in healthcare?
ROI, or "Return on Investment," is a term that gets bandied about frequently in healthcare, particularly when it comes to providers assessing whether their new, expensive IT systems are "paying off."
What is required for release of information in healthcare?
The core elements of a valid authorization include: A meaningful description of the information to be disclosed. The name of the individual or the name of the person authorized to make the requested disclosure. The name or other identification of the recipient of the information.
What is the proper way for a patient to bring about the release of health records quizlet?
The patient must sign an authorization to release records. Use in a Court of Law. When a subpoena duces tecum is issued for certain records (subpoena commands a witness to appear in court and to bring certain medical records), the patient's written consent to release the records is waived.
How do medical releases work?
A medical records release form is a document that allows you to share patient information with an outside party, such as an employer, an insurance company, a family member, another doctor or healthcare provider, or other third party.
What is a medical authorization?
A decision by your health insurer or plan that a health care service, treatment plan, prescription drug or durable medical equipment is medically necessary. Sometimes called prior authorization, prior approval or precertification.
What is the best way to request the release of medical information?
You may be able to request your record through your provider's patient portal. You may have to fill out a form — called a health or medical record release form, or request for access—send an email, or mail or fax a letter to your provider.
What is the importance of the release of information form?
A release of information is a document that gives a consumer the opportunity to decide what material they want released from their medical file, who they want it delivered to, how long the data can be issued, and under what statutes and guidelines it is released.
What is a medical release authorization?
This form is to authorize a medical doctor or nurse practitioner to release medical information. The patient or their legally authorized representative must. complete and sign this form and show it to the medical doctor or nurse practitioner who will complete and sign the Medical Certificate for Employment Insurance.
Which of the following people can authorize the release of a patient's medical information?
Under HIPAA, a "personal representative" is the person who has authority to make healthcare decisions for the patient under applicable state law. (45 CFR 164.502(g)(2)-(3)). A personal representative generally has the right to access or authorize disclosures of information just like the patient.
What are the steps of the release of information process?
Phase 1: Recording, Tracking and Verifying the Request. Phase 2: Retrieving Your PHI. Phase 3: Safeguarding Your Sensitive Information. Phase 4: Releasing Your PHI. Phase 5: Completing the Request and Preparing an Invoice.
Who controls the release of patient information?
Hospitals and health systems are responsible for protecting the privacy and confidentiality of their patients and patient information. The Health Insurance Portability and Accountability Act of 1996 (HIPAA) regulations established national privacy standards for health care information.
What is a release of authorization?
By setting up a Release Authorization (ARI), you are giving customer service your permission to disclose information about your accounts to another person. Typically, this is used to give account access to a spouse or other family member.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I make changes in mr 54302 patient authorization?
The editing procedure is simple with pdfFiller. Open your mr 54302 patient authorization in the editor. You may also add photos, draw arrows and lines, insert sticky notes and text boxes, and more.
Can I create an electronic signature for signing my mr 54302 patient authorization in Gmail?
It's easy to make your eSignature with pdfFiller, and then you can sign your mr 54302 patient authorization right from your Gmail inbox with the help of pdfFiller's add-on for Gmail. This is a very important point: You must sign up for an account so that you can save your signatures and signed documents.
How do I fill out the mr 54302 patient authorization form on my smartphone?
Use the pdfFiller mobile app to fill out and sign mr 54302 patient authorization. Visit our website (https://edit-pdf-ios-android.pdffiller.com/) to learn more about our mobile applications, their features, and how to get started.
What is PA MR 543.02?
PA MR 543.02 is a form used for reporting specific tax-related information to the Pennsylvania Department of Revenue.
Who is required to file PA MR 543.02?
Individuals or businesses that meet certain tax criteria set by the Pennsylvania Department of Revenue are required to file PA MR 543.02.
How to fill out PA MR 543.02?
To fill out PA MR 543.02, gather the necessary tax information, complete all required sections on the form accurately, and submit it to the Pennsylvania Department of Revenue by the specified deadline.
What is the purpose of PA MR 543.02?
The purpose of PA MR 543.02 is to collect important tax information to ensure compliance with Pennsylvania tax laws and to assist in the assessment of tax liabilities.
What information must be reported on PA MR 543.02?
PA MR 543.02 requires the reporting of information such as income, deductions, credits, and any other relevant financial data specified by the Pennsylvania Department of Revenue.
Fill out your mr 54302 patient authorization online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Mr 54302 Patient Authorization is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
