Last updated on Apr 10, 2026
Get the free Provider Appeal Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
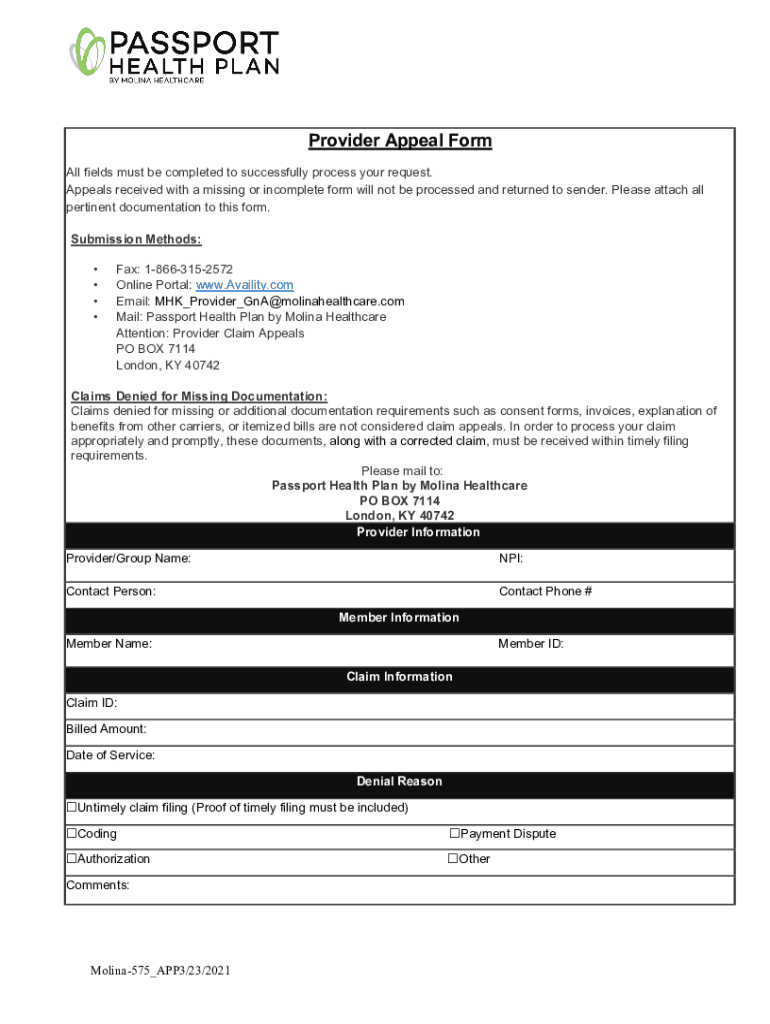
What is provider appeal form
The Provider Appeal Form is a healthcare document used by providers to appeal denied claims with Molina Healthcare.
pdfFiller scores top ratings on review platforms
Who needs provider appeal form?
Explore how professionals across industries use pdfFiller.

Provider appeal form is needed by:
-
Healthcare providers seeking to challenge claim denials
-
Billing specialists managing claims for healthcare entities
-
Insurance coordinators handling appeals and claims
-
Members or patients wanting to understand their claims
-
Administrative staff involved in healthcare compliance
-
Legal representatives supporting providers with claims
Comprehensive Guide to provider appeal form
What is the Provider Appeal Form?
The Provider Appeal Form is crucial for healthcare providers as it allows them to contest denied claims with Molina Healthcare. This form serves as a formal request to review decisions made on claims, enhancing access to financial resources. Any eligible healthcare provider can utilize this form, especially when faced with common scenarios such as claim denials.
This form is not just a standard document; it represents an avenue for providers to advocate for fair treatment and reimbursement within the healthcare system. Each submission can significantly impact a provider's financial stability, making understanding this process essential.
Purpose and Benefits of the Provider Appeal Form
The Provider Appeal Form holds significant advantages for healthcare providers, primarily through the potential of improving financial outcomes by appealing denied claims. This form also streamlines communication with insurance providers, ensuring that discrepancies are addressed effectively.
Utilizing the form can lead to more favorable resolutions and a better understanding of claim processes, which is integral for maintaining good relationships between providers and insurance companies.
Who Needs the Provider Appeal Form?
This form is designed for a variety of healthcare providers, including hospitals and clinics that experience claim denials. Understanding the eligibility criteria for filing an appeal is essential for ensuring that the process is effective and timely.
Healthcare entities that wish to challenge claims must possess the requisite understanding of their rights and obligations within the appeals process. This empowers them to engage with the system more effectively.
When and How to Submit the Provider Appeal Form
Timely filing of the Provider Appeal Form is critical, as late submissions can jeopardize the appeal process, leading to automatic denials. Providers can submit this form through several channels, ensuring flexibility in how they handle their appeals.
-
Fax: Quick transmission of documents for immediate processing.
-
Online portal: A convenient way to submit and track appeals digitally.
-
Email: Allows for a written record of submissions.
-
Mail: Traditional method for sending documents.
Required Documents and Supporting Materials
To support the appeal effectively, providers must include specific documentation with their submission. Providing thorough and accurate information is essential for increasing the chances of a favorable outcome.
-
Denial letters from Molina Healthcare.
-
Supporting clinical documentation relevant to the claim.
-
Any previous correspondence related to the claim.
How to Fill Out the Provider Appeal Form Online (Step-by-Step)
Filling out the Provider Appeal Form online can enhance efficiency using tools like pdfFiller. Follow these steps to ensure a complete and accurate submission.
-
Access the Provider Appeal Form through the pdfFiller platform.
-
Complete the required fields, such as provider and member information.
-
Include the denial reason and supporting materials.
-
Review your entries to confirm accuracy.
-
Submit the form through your preferred channel.
Common Errors and How to Avoid Them
Many appeals face rejection due to common errors made during the completion of the Provider Appeal Form. Identifying these can minimize mistakes and enhance approval rates.
-
Leaving fields incomplete or providing ambiguous information.
-
Failing to attach necessary supporting documentation.
-
Submitting after the designated timeline for appeals.
What Happens After You Submit the Provider Appeal Form?
Once the Provider Appeal Form is submitted, providers can expect a specific post-submission process regarding the status of their appeal. It is crucial to understand how to track the appeal and anticipate possible outcomes.
-
A confirmation will typically be sent acknowledging receipt of the appeal.
-
The timeframe for receiving a decision may vary based on the complexity of the claim.
Security and Compliance When Using the Provider Appeal Form
Handling sensitive patient information demands strict adherence to security protocols. When using the Provider Appeal Form, providers must prioritize privacy and compliance with established regulations.
pdfFiller implements robust security measures, including 256-bit encryption and compliance with HIPAA guidelines, ensuring the protection of sensitive healthcare data throughout the appeal process.
Get Started with pdfFiller to Complete Your Provider Appeal Form
Utilizing pdfFiller simplifies the process of completing the Provider Appeal Form. With features designed for efficiency, such as eSigning and secure cloud storage, users can manage their healthcare forms with ease.
With its user-friendly interface and strong security measures, pdfFiller stands out as an essential tool for healthcare providers looking to navigate the appeals process effectively.
How to fill out the provider appeal form
-
1.To access the Provider Appeal Form on pdfFiller, visit the platform’s website and search for 'Provider Appeal Form' in the search bar.
-
2.Once located, click on the form to open it in the pdfFiller editor, allowing you to interact with the fillable fields directly.
-
3.Before completing the form, gather all necessary information, including provider details, member specifics, claims information, and the reason for denial, along with any supporting documentation.
-
4.Navigate through the form by clicking on each fillable field. Enter the required information accurately and ensure you complete every section as instructed.
-
5.Use the checkboxes where appropriate, and refer to any detailed instructions included within the form to avoid errors.
-
6.Review all entered information for accuracy, ensuring that every field is completed, as incomplete forms may not be processed.
-
7.Once satisfied with your entries, finalize the form using pdfFiller’s options, such as adding your electronic signature if required.
-
8.Finally, save or download your completed form. You can submit it directly through pdfFiller if an online portal for submission is available.

Who is eligible to use the Provider Appeal Form?
The Provider Appeal Form is designed for healthcare providers who have had claims denied by Molina Healthcare and wish to appeal those decisions.
What is the deadline for submitting the appeal?
Appeals must be submitted within the timely filing requirements set by Molina Healthcare. It's crucial to check their precise deadlines to ensure your appeal is processed.
How can I submit the completed Provider Appeal Form?
You can submit the completed Provider Appeal Form via fax, online portal, email, or mail it to the designated address in London, KY. Ensure you choose the method that meets your timeline.
What supporting documents are required with the form?
You should include any relevant supporting documentation that provides context and evidence for your appeal, such as denial letters and detailed claims information.
What are common mistakes to avoid when filling out the form?
Ensure all fields are completed, particularly those related to the denial reason and claim information. Failing to furnish complete information can delay the processing of your appeal.
How long does it take to process the appeal?
Processing times for claims appeals can vary. Typically, it may take several weeks, so be sure to follow up if you do not receive a response within a reasonable time frame.
Is notarization required for the Provider Appeal Form?
No, notarization is not required for the Provider Appeal Form, making it easier for healthcare providers to submit their appeals without additional formalities.
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.