Last updated on Apr 10, 2026
Get the free 2021 Annual Consent Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is 2021 annual consent form
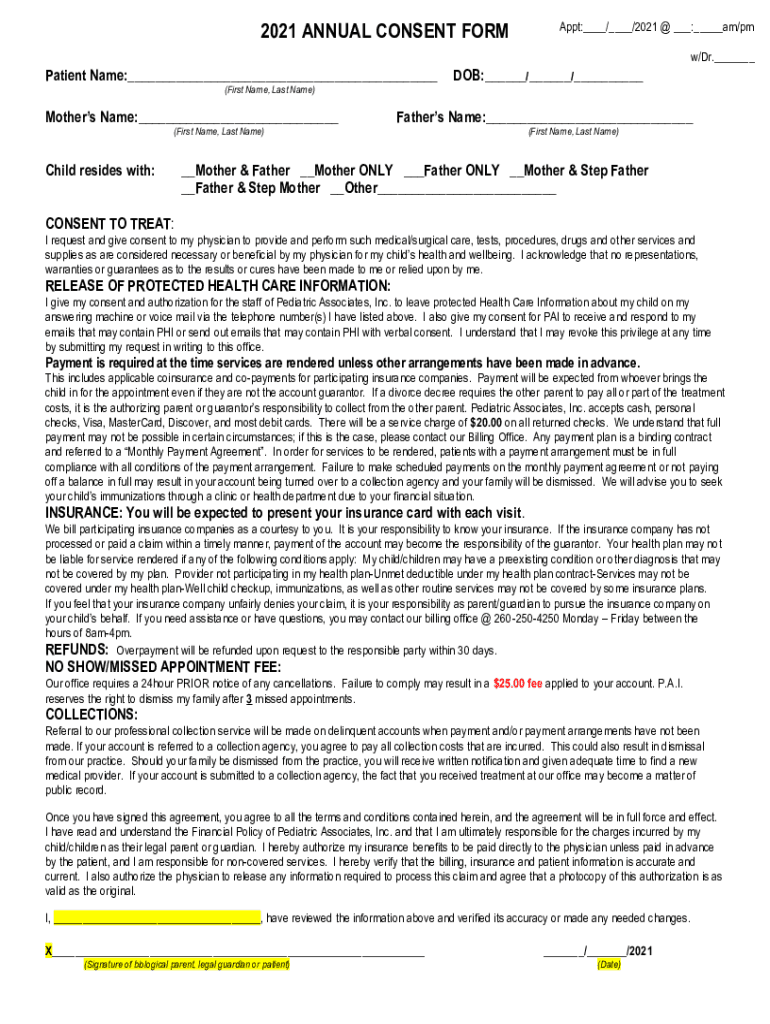
The 2021 Annual Consent Form is a medical consent document used by Pediatric Associates, Inc. to obtain necessary authorizations from parents or legal guardians regarding medical treatment and the release of protected health information.
pdfFiller scores top ratings on review platforms
Who needs 2021 annual consent form?
Explore how professionals across industries use pdfFiller.

2021 annual consent form is needed by:
-
Parents or legal guardians of pediatric patients
-
Medical practitioners at Pediatric Associates, Inc.
-
Healthcare personnel involved in patient treatment
-
Insurance providers requiring treatment authorization
-
Administrative staff managing patient records
-
Individuals involved in the healthcare decision-making process
Comprehensive Guide to 2021 annual consent form
What is the 2021 Annual Consent Form?
The 2021 Annual Consent Form is a crucial document used by Pediatric Associates, Inc. to obtain consent for medical treatment and to release protected health information. This form holds significant importance in healthcare settings, particularly for pediatric care, ensuring that parents or legal guardians grant permission for their child's medical treatment.
Key terms such as patient consent, medical treatment consent, and HIPAA authorization are integral to understanding this form. It provides necessary legal backing for treatments and protects sensitive patient health information.
Purpose and Benefits of the 2021 Annual Consent Form
This form is essential for pediatric care, as it formalizes the process whereby parents or legal guardians provide approval for medical treatment. By using the 2021 Annual Consent Form, caregivers ensure that they are legally authorized to approve treatments, which can facilitate smoother interactions with healthcare providers.
Additionally, this form aids in the authorization process regarding insurance billing, ensuring that claims can be processed efficiently. Using a healthcare authorization form guarantees that all parties are on the same page when it comes to treatment approvals.
Key Features of the 2021 Annual Consent Form
The 2021 Annual Consent Form includes several critical components designed to ensure comprehensive documentation. It consists of fillable fields where users can input vital information about the patient, treatment consent, and HIPAA authorization.
Benefits of using a digital patient consent form include increased accessibility and a streamlined process. Compared to traditional paper forms, a digital format allows for easier editing and sharing, enhancing the overall experience for parents and healthcare providers alike. Features such as checkboxes help clarify the scope of consent and specific authorizations.
Who Needs the 2021 Annual Consent Form?
The primary target audience for the 2021 Annual Consent Form includes parents or legal guardians of minors. Healthcare professionals may also require this consent to ensure compliance when providing treatment. Situations that necessitate filling out this form typically arise in Indiana, particularly when medical treatment for a child is being considered.
How to Fill Out the 2021 Annual Consent Form Online (Step-by-Step)
-
Access the form on pdfFiller.
-
Begin by filling in the patient’s details, which include the Patient Name and Date of Birth (DOB).
-
Enter guardian information, such as Mother’s and Father’s names.
-
Review the provided information for accuracy before proceeding.
-
Submit the form securely after signing digitally, ensuring all sensitive information is carefully handled.
Signing and Submitting the 2021 Annual Consent Form
There are several options for signing the 2021 Annual Consent Form, including both digital and wet signature methods. Once completed, submission can occur online through pdfFiller or via traditional mail to the appropriate healthcare provider.
Prior to submission, it is vital to ensure that all sections of the form are complete to avoid any potential delays in treatment approvals.
Consequences of Not Filing or Late Filing the 2021 Annual Consent Form
Failure to file the 2021 Annual Consent Form or submitting it late can lead to significant delays in medical treatment for the child. Legally, parents or guardians may face implications if consent is not provided, emphasizing the necessity of timely submission.
Understanding rights regarding medical consent is essential for parents and guardians to navigate these legal responsibilities effectively.
Security and Compliance for the 2021 Annual Consent Form
Data protection is paramount when managing sensitive health information contained within the 2021 Annual Consent Form. pdfFiller employs robust security measures, including 256-bit encryption and ensuring HIPAA compliance, to safeguard user data.
Parents should remain vigilant about data security by using verified platforms like pdfFiller, further ensuring that their sensitive documents are handled with care.
How pdfFiller Can Help with the 2021 Annual Consent Form
pdfFiller enhances the form-filling experience for users, offering benefits such as easy editing, signing, and sharing of the 2021 Annual Consent Form. By utilizing pdfFiller, parents can efficiently manage their documents while ensuring compliance and security standards are met.
Get Started with the 2021 Annual Consent Form Today!
Users can begin the process of filling out the 2021 Annual Consent Form using pdfFiller, which promotes an easy and secure experience. Accurate completion of the form is critical, and the online platform facilitates this by providing seamless document management solutions.
How to fill out the 2021 annual consent form
-
1.Access pdfFiller and search for '2021 Annual Consent Form' in the search bar.
-
2.Select the form and click on 'Open in Editor' to begin filling out the form.
-
3.Before starting, gather all necessary information, including patient details like name, date of birth, and guardian information.
-
4.Fill in the 'Patient Name' and 'DOB' fields with the child's details, ensuring accuracy.
-
5.In the sections for parental information, enter the names of the mother and father as required.
-
6.Use the checkboxes to indicate the child's living situation, marking the appropriate option.
-
7.Review each section to ensure all required fields are filled accurately, especially the consent for treatment and insurance billing sections.
-
8.Sign the form where indicated, ensuring that the signature matches the name of the signing parent or guardian.
-
9.After completing the form, review it one last time for any errors or omissions.
-
10.To save or download the form, click on the 'Save' or 'Download' button and choose your preferred file format.
-
11.If necessary, you can submit the completed form directly through pdfFiller or print it to send via mail or in-person.

Who is eligible to complete the 2021 Annual Consent Form?
The 2021 Annual Consent Form must be completed by a parent or legal guardian of the minor patient. This ensures that only authorized individuals can consent to medical treatment and release of information.
What is the deadline for submitting this consent form?
While specific deadlines may vary, it is typically recommended to submit the 2021 Annual Consent Form before the child's scheduled medical appointment to ensure timely processing.
How can I submit the completed 2021 Annual Consent Form?
You can submit the completed form through pdfFiller, where you may have options to save, download, or submit it electronically. Alternatively, printed forms can be submitted by mail or delivered in person.
What supporting documents are required with this form?
Typically, no additional supporting documents are required with the 2021 Annual Consent Form. However, it is essential to accurately complete all relevant fields to avoid processing delays.
What common mistakes should I avoid when filling out this form?
Ensure all fields are completely and accurately filled, especially patient identifying information and signatures. Leaving important fields blank or providing incorrect details can result in delays.
How long does it take to process the consent form?
Processing times for the 2021 Annual Consent Form usually depend on the administrative procedures of the healthcare facility. Generally, approval is quick if all details are correct and forms are timely submitted.
What if I need to make changes after submitting the form?
If changes are needed after submission, contact Pediatric Associates, Inc. directly to inquire about the procedure for amending the consent information on file.
Related Forms








Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.