Get the free docs.medaviebc.caprovidersformsPROVIDER CLAIM FORM - docs.medaviebc.ca
Show details
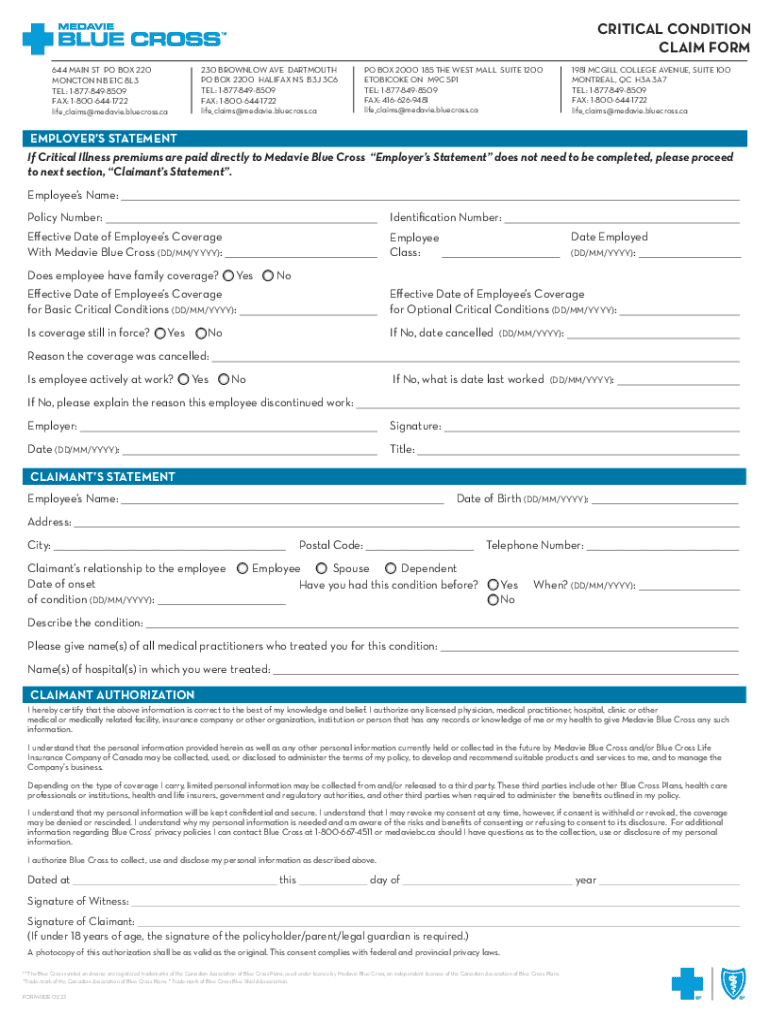
CRITICAL CONDITION CLAIM FORM 644 MAIN ST PO BOX 220 MONCTON NB E1C 8L3 TEL: 18778498509 FAX: 18006441722 life×claims×Melanie.blue cross.ca230 BROWNLOW AVE DARTMOUTH PO BOX 2200 HALIFAX NS B3J 3C6
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign docsmedaviebccaprovidersformsprovider claim form
Edit your docsmedaviebccaprovidersformsprovider claim form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your docsmedaviebccaprovidersformsprovider claim form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing docsmedaviebccaprovidersformsprovider claim form online



Use the instructions below to start using our professional PDF editor:
1
Register the account. Begin by clicking Start Free Trial and create a profile if you are a new user.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit docsmedaviebccaprovidersformsprovider claim form. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Get your file. When you find your file in the docs list, click on its name and choose how you want to save it. To get the PDF, you can save it, send an email with it, or move it to the cloud.
pdfFiller makes dealing with documents a breeze. Create an account to find out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out docsmedaviebccaprovidersformsprovider claim form
How to fill out docsmedaviebccaprovidersformsprovider claim form
01
To fill out the docsmedaviebccaprovidersformsprovider claim form, follow these steps:
02
Start by writing the patient's personal information, such as their name, address, and contact details, in the designated fields.
03
Next, provide the patient's insurance information, including their policy number and any group or plan numbers.
04
Specify the dates of service for which the claim is being submitted.
05
Enter the details of the healthcare services rendered, including the name of the provider, the service codes, and any fees or charges associated with each service.
06
Include any supporting documentation, such as itemized bills or medical reports, that may be required for claim processing.
07
Sign and date the form to certify that the information provided is accurate and complete.
08
Make a copy of the completed form for your records before submitting it to the appropriate claims department or mailing address.
09
Remember to follow any additional instructions or requirements mentioned on the claim form or provided by the insurance provider.
10
Following these steps will ensure that you correctly fill out the docsmedaviebccaprovidersformsprovider claim form.
Who needs docsmedaviebccaprovidersformsprovider claim form?
01
The docsmedaviebccaprovidersformsprovider claim form is typically needed by healthcare providers who have rendered services to patients covered under Medavie Blue Cross insurance. This form is used to submit claims for reimbursement or payment for the healthcare services provided. It is required by healthcare professionals, such as doctors, specialists, therapists, and hospitals, who want to seek compensation for their services from Medavie Blue Cross.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I complete docsmedaviebccaprovidersformsprovider claim form online?
Completing and signing docsmedaviebccaprovidersformsprovider claim form online is easy with pdfFiller. It enables you to edit original PDF content, highlight, blackout, erase and type text anywhere on a page, legally eSign your form, and much more. Create your free account and manage professional documents on the web.
How do I edit docsmedaviebccaprovidersformsprovider claim form straight from my smartphone?
The pdfFiller apps for iOS and Android smartphones are available in the Apple Store and Google Play Store. You may also get the program at https://edit-pdf-ios-android.pdffiller.com/. Open the web app, sign in, and start editing docsmedaviebccaprovidersformsprovider claim form.
Can I edit docsmedaviebccaprovidersformsprovider claim form on an Android device?
The pdfFiller app for Android allows you to edit PDF files like docsmedaviebccaprovidersformsprovider claim form. Mobile document editing, signing, and sending. Install the app to ease document management anywhere.
What is docsmedaviebccaprovidersformsprovider claim form?
The docsmedaviebccaprovidersformsprovider claim form is a form used for submitting claims to providers for services rendered.
Who is required to file docsmedaviebccaprovidersformsprovider claim form?
Healthcare providers are required to file the docsmedaviebccaprovidersformsprovider claim form for reimbursement of services provided.
How to fill out docsmedaviebccaprovidersformsprovider claim form?
The docsmedaviebccaprovidersformsprovider claim form should be filled out accurately and completely with all relevant information about the patient, services provided, and any supporting documentation.
What is the purpose of docsmedaviebccaprovidersformsprovider claim form?
The purpose of the docsmedaviebccaprovidersformsprovider claim form is to request reimbursement for healthcare services provided.
What information must be reported on docsmedaviebccaprovidersformsprovider claim form?
The docsmedaviebccaprovidersformsprovider claim form must include information such as patient details, service provided, date of service, provider information, and any supporting documentation.
Fill out your docsmedaviebccaprovidersformsprovider claim form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Docsmedaviebccaprovidersformsprovider Claim Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
