Last updated on May 26, 2026
Get the free Patient Medical History Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Patient Medical History Form
The Patient Medical History Form is a healthcare document used by providers to collect comprehensive medical information from patients before treatment.
pdfFiller scores top ratings on review platforms
Who needs Patient Medical History Form?
Explore how professionals across industries use pdfFiller.

Patient Medical History Form is needed by:
-
Patients seeking medical treatment
-
Healthcare providers conducting patient consultations
-
Medical professionals assessing patient history
-
Aesthetic treatment facilities like AesthetiSpa
-
Insurance companies verifying medical claims
-
Clinical researchers collecting patient data
Comprehensive Guide to Patient Medical History Form
What is the Patient Medical History Form?
The Patient Medical History Form is a crucial document used in healthcare settings to collect detailed medical information from patients prior to treatment. This form plays an essential role in medical treatments by ensuring that healthcare providers have access to accurate and comprehensive patient data.
It collects various types of information, including personal details, medical history, and treatment preferences. By documenting this information accurately, the form helps both patients and healthcare providers effectively participate in the treatment process.
Purpose and Benefits of Using the Patient Medical History Form
The Patient Medical History Form offers significant advantages for both patients and healthcare providers during the treatment process. For patients, this form ensures they provide accurate medical information, which is vital for receiving appropriate treatment.
Healthcare providers benefit from the information gathered through the form as it aids in informed decision-making and treatment planning. By prioritizing comprehensive information gathering, the form helps enhance patient care and safety throughout the treatment journey.
Key Features of the Patient Medical History Form
This form is composed of several key sections designed to gather essential information, including personal details, current medical conditions, and skin history. Each section contains fillable fields and checkboxes to streamline the data collection process.
Additionally, both patient and provider signatures are required for validation, underscoring the importance of accuracy and accountability in the information provided.
Who Needs the Patient Medical History Form?
The Patient Medical History Form is primarily required for patients seeking treatment at healthcare facilities, such as AesthetiSpa, Inc. Healthcare providers also rely on this form as an effective tool for gathering comprehensive medical histories from patients.
Situations where this form is essential include initial consultations, ongoing treatments, and any instances where a complete patient medical history is necessary for safe and effective care.
How to Fill Out the Patient Medical History Form Online
To efficiently complete the Patient Medical History Form online, follow these clear steps:
-
Access the form through pdfFiller’s platform.
-
Fill out each section, providing required information as indicated in the fillable fields.
-
Review your entries for accuracy to avoid submission errors.
Ensuring accurate and complete submissions is crucial for maintaining effective communication between patients and healthcare providers.
Submitting the Patient Medical History Form
Once you have completed the Patient Medical History Form, you can choose from several submission methods, including online submission through pdfFiller, sending via email, or delivering it directly to your healthcare provider.
Be aware of any potential fees, deadlines, and processing times associated with your submission. Additionally, confirmation and tracking options may be available to verify the successful submission of your form.
How pdfFiller Helps with Your Patient Medical History Form
Utilizing pdfFiller for managing the Patient Medical History Form offers numerous advantages, such as editing capabilities, eSigning features, and efficient form management tools. This platform enables users to easily create and modify forms tailored to their needs.
Security measures such as 256-bit encryption and HIPAA compliance ensure that all sensitive data is protected. Users have successfully submitted their forms via pdfFiller, noting its ease of use and reliability in handling medical documents.
Privacy and Security with the Patient Medical History Form
Data protection is paramount when dealing with patient information, and pdfFiller provides assurances of confidentiality through robust security measures. Compliance with HIPAA regulations further underscores the importance of safeguarding sensitive medical data.
Using secure tools for handling patient information is highly encouraged to protect privacy and prevent unauthorized access to medical records.
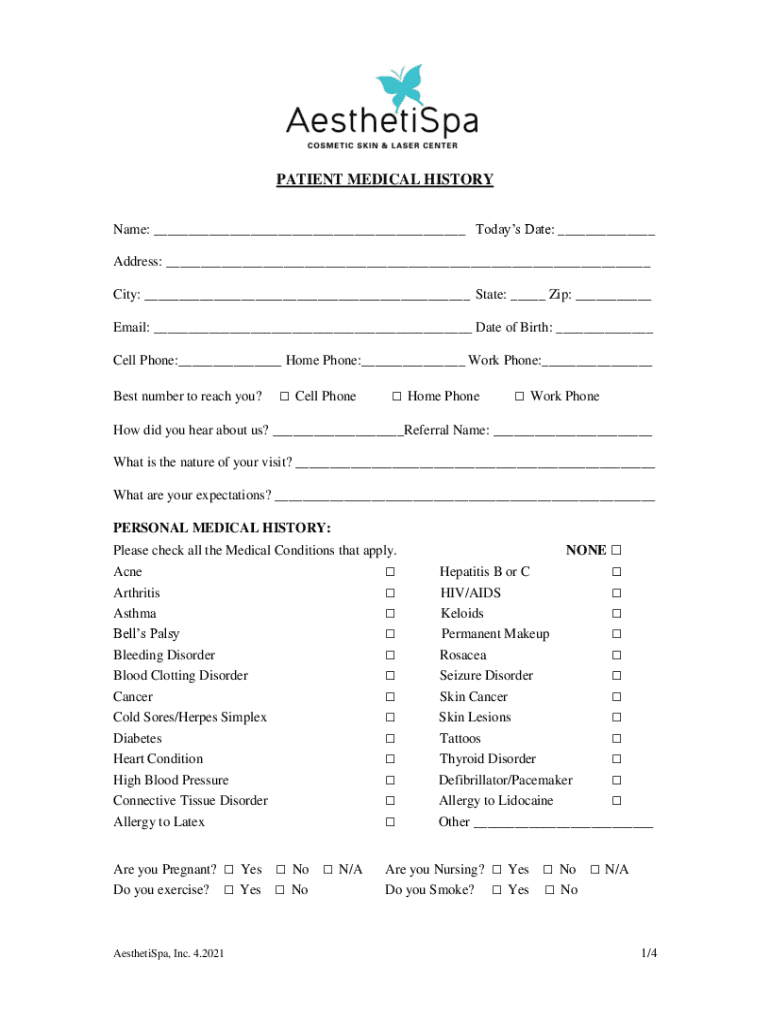
Sample Patient Medical History Form
A visual representation of a completed Patient Medical History Form illustrates the types of information collected and highlights key areas that require attention. This sample can serve as a valuable reference for users.
Additionally, templates available on pdfFiller facilitate users in creating their forms, showcasing the importance of well-documented patient medical history.
Getting Started with pdfFiller Today
Begin your journey by creating an account on pdfFiller to access the Patient Medical History Form. The platform is designed for ease of use, allowing users to fill out forms directly without the need for downloads.
Take advantage of the editing and eSigning features to streamline the process of completing your medical history documentation, ensuring a smooth experience from start to finish.
How to fill out the Patient Medical History Form
-
1.To access the Patient Medical History Form on pdfFiller, visit the pdfFiller website and log in to your account or create a new account if you do not have one.
-
2.Once logged in, type 'Patient Medical History Form' in the search bar to locate the form quickly.
-
3.Click on the form title to open it in the pdfFiller editor, where you can view and fill out the necessary fields smoothly.
-
4.Before starting to fill out the form, gather necessary information such as personal details, current medications, and medical history by reviewing your health records or consulting with a healthcare professional.
-
5.Navigate through the form using the pdfFiller interface, which allows you to click on fillable fields and type in your responses directly.
-
6.Use the tabs or scroll through the document to access different sections, which include personal information, medical conditions, and treatment preferences.
-
7.Ensure that you complete all required fields marked with an asterisk (*) and review the form for accuracy.
-
8.Once you have filled out all sections, double-check your entries for completeness and correctness.
-
9.After reviewing, proceed to finalize the form by selecting the 'Save' option to preserve your work.
-
10.To download or submit the completed form, click on the 'Download' button to save it to your device or use the 'Submit' option to directly send it to the healthcare provider.

Who needs to fill out the Patient Medical History Form?
Patients who are seeking medical treatment or cosmetic procedures need to fill out the Patient Medical History Form to provide healthcare providers with vital medical background.
Is there a deadline for submitting the Patient Medical History Form?
It's advisable to submit the Patient Medical History Form prior to your scheduled appointment. Check with your healthcare provider for any specific submission deadlines.
How should I submit the completed form?
The completed Patient Medical History Form can be submitted online through pdfFiller by utilizing the 'Submit' option or downloaded and sent via email to your healthcare provider, depending on their procedures.
What supporting documents are required with this form?
Typically, you may need to provide identification, insurance details, and any previous medical records that support information filled in the Patient Medical History Form.
What are common mistakes to avoid when completing the form?
Common mistakes include leaving required fields blank, providing inaccurate information, or failing to sign both the patient's and provider's signature sections.
How long does it take to process the Patient Medical History Form?
Processing time can vary but typically, once submitted, your healthcare provider will review your form and respond within a few business days.
Can I edit the Patient Medical History Form after submission?
Once submitted, the Patient Medical History Form typically cannot be edited. If changes are necessary, contact your healthcare provider immediately to discuss the updates required.
Related Forms







Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.