
Get the free Part B KY & OH Overpayment Recovery Request
Show details
Este formulario debe utilizarse para iniciar un ajuste por un reclamo pagado en exceso. Esto podría ser por artículos devueltos, error de facturación o por sobrepagos que involucran Medicare Payer
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign part b ky oh
Edit your part b ky oh form online
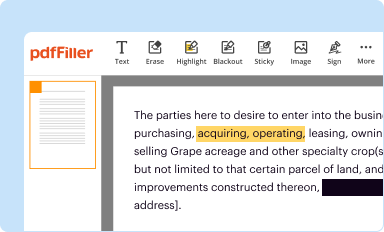
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
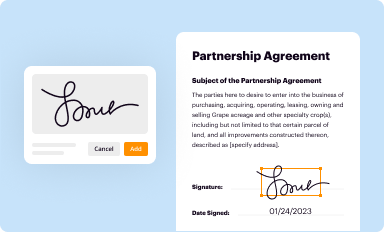
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
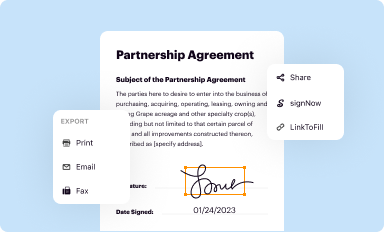
Share your form instantly
Email, fax, or share your part b ky oh form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit part b ky oh online



Use the instructions below to start using our professional PDF editor:
1
Sign into your account. If you don't have a profile yet, click Start Free Trial and sign up for one.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit part b ky oh. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
It's easier to work with documents with pdfFiller than you can have ever thought. You can sign up for an account to see for yourself.
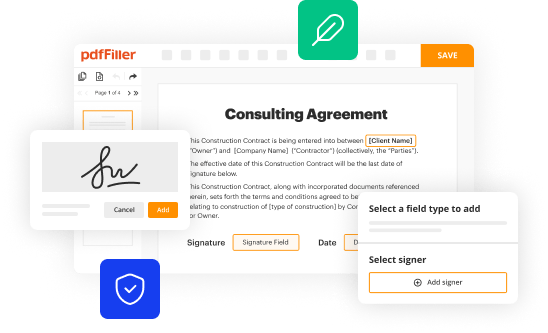
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out part b ky oh
How to fill out Part B KY & OH Overpayment Recovery Request
01
Gather necessary documents: Ensure you have all relevant information and documents related to the overpayment.
02
Access the form: Obtain the Part B KY & OH Overpayment Recovery Request form from the relevant agency's website or office.
03
Fill in personal information: Enter your name, address, contact information, and Medicare number accurately at the top of the form.
04
Provide details of the overpayment: Clearly specify the overpayment amount, dates, and reasons provided by the agency.
05
Attach supporting documents: Include any documentation that supports your claim regarding the overpayment.
06
Review the form: Double-check all entered information for accuracy and completeness.
07
Sign and date the form: Ensure you sign and date the request before submission.
08
Submit the form: Send the completed form to the address specified in the instructions, using a reliable mailing method.
Who needs Part B KY & OH Overpayment Recovery Request?
01
Individuals who have received notice of an overpayment for Medicare Part B services in Kentucky or Ohio.
02
Beneficiaries who want to formally request a review or recovery of the overpayment amount.
Fill
form
: Try Risk Free
People Also Ask about
Does Medicare refund premium overpayments?
No. An employer can only claim a refund of overpaid Additional Medicare Tax if it did not deduct or withhold the overpaid Additional Medicare Tax from the employee's wages.
Do you get a refund if you overpaid Medicare tax?
Recoupments by Medicare Advantage plans are regulated by federal law. Under federal law, plans can request a refund for any reason within one year of the date of the payment and within four years from the date of the payment, for good cause.
How do I get a refund from Medicare overpayment?
A voluntary refund is when an overpayment has been self-identified. A check is required to be submitted along with the appropriate form. The check will be applied to the identified overpayments. If there are excess funds, they will be applied per CMS Medicare Learning Network (MLN) Matters (MM) 3274.
How to refund Medicare for overpayment?
Submit a Voluntary Refund Complete MSP Voluntary Checks Form in its entirety. Indicate appropriate reason code for claim adjustment on MSP Voluntary Checks Form. Include a check along with primary insurer EOB. Mail MSP Voluntary Checks Form to address provided on form.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I modify my part b ky oh in Gmail?
In your inbox, you may use pdfFiller's add-on for Gmail to generate, modify, fill out, and eSign your part b ky oh and any other papers you receive, all without leaving the program. Install pdfFiller for Gmail from the Google Workspace Marketplace by visiting this link. Take away the need for time-consuming procedures and handle your papers and eSignatures with ease.
How do I edit part b ky oh straight from my smartphone?
Using pdfFiller's mobile-native applications for iOS and Android is the simplest method to edit documents on a mobile device. You may get them from the Apple App Store and Google Play, respectively. More information on the apps may be found here. Install the program and log in to begin editing part b ky oh.
How do I fill out part b ky oh on an Android device?
Complete part b ky oh and other documents on your Android device with the pdfFiller app. The software allows you to modify information, eSign, annotate, and share files. You may view your papers from anywhere with an internet connection.
What is Part B KY & OH Overpayment Recovery Request?
The Part B KY & OH Overpayment Recovery Request is a formal process used by Medicare providers in Kentucky and Ohio to request recovery of overpayments made by Medicare for Part B services.
Who is required to file Part B KY & OH Overpayment Recovery Request?
Medicare providers who have received overpayments for Part B services in Kentucky and Ohio are required to file this request.
How to fill out Part B KY & OH Overpayment Recovery Request?
To fill out the Part B KY & OH Overpayment Recovery Request, providers must complete the designated form available from the Medicare website or their local Medicare Administrative Contractor, providing all necessary information as indicated in the form instructions.
What is the purpose of Part B KY & OH Overpayment Recovery Request?
The purpose of the Part B KY & OH Overpayment Recovery Request is to allow providers to formally alert Medicare of any identified overpayments and initiate the process for recovery of those funds.
What information must be reported on Part B KY & OH Overpayment Recovery Request?
The information required includes the provider's identification details, specifics about the overpayment (such as claim numbers and amounts), and a statement explaining the reason for the overpayment.
Fill out your part b ky oh online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Part B Ky Oh is not the form you're looking for?Search for another form here.
Relevant keywords
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
